

Determining the frequency of de novo germline mutations in DNA mismatch repair genes
- PMID: 21636617
- PMCID: PMC3436601
- DOI: 10.1136/jmedgenet-2011-100082
Determining the frequency of de novo germline mutations in DNA mismatch repair genes
Abstract
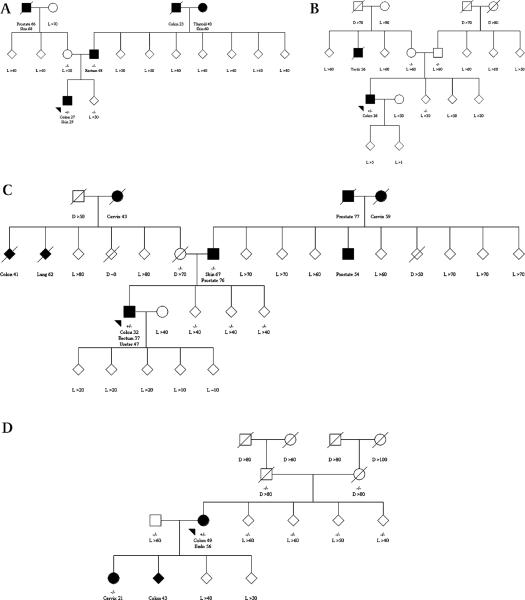
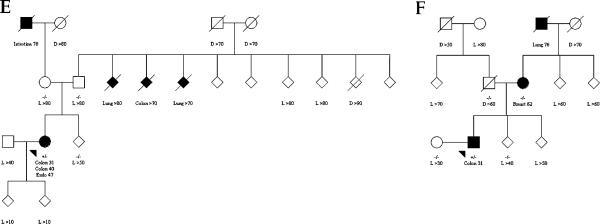
Background: Carriers of a germline mutation in a DNA mismatch repair (MMR) gene--that is, persons with Lynch syndrome--have substantially high risks of colorectal (CRC), endometrial, and several other cancers. The proportion of carriers who have de novo mutations (not inherited from either parent) is not known. This study reports a case series of de novo mutations in MMR genes and estimates the frequency of de novo mutation in MMR genes using the Colon Cancer Family Registry.
Methods: Screening for germline MLH1, MSH2, MSH6, and PMS2 mutations was performed for all incident CRC cases recruited from cancer registries (population based probands) displaying microsatellite instability (MSI) or loss of expression of MMR genes by immunohistochemistry (IHC) and probands with CRC in multi-case families recruited from clinics (clinic based probands), regardless of MSI or IHC status. All relatives of probands with a pathogenic mutation who donated a blood sample underwent testing for the mutation identified in the proband.
Results: Of 261 probands (202 clinic based, 59 population based) with MMR gene mutations for whom it was possible to determine the origin of the mutation, six (2.3%, 95% CI 0.9% to 5.0%) were confirmed as de novo, and the remaining 255 (97.7%, 95% CI 95.0% to 99.1%) were inherited. Of the de novo mutation carriers, three were clinic based probands (1.5%, 95% CI 0.3% to 4.5%) and three were population based probands (5.1%, 95% CI 1.2% to 14.5%). Two were in MLH1, three in MSH2, and one in MSH6.
Conclusion: De novo MMR gene mutations are uncommon causes of Lynch syndrome.
Figures
References
-
- Vasen HF. Clinical diagnosis and management of hereditary colorectal cancer syndromes. J Clin Oncol. 2000;18:81S–92S. - PubMed
-
- Muller A, Fishel R. Mismatch repair and the hereditary non-polyposis colorectal cancer syndrome (HNPCC) Cancer Invest. 2002;20:102–9. - PubMed
-
- Baglietto L, Lindor NM, Dowty JG, White DM, Wagner A, Gomez Garcia EB, Vriends AH, Cartwright NR, Barnetson RA, Farrington SM, Tenesa A, Hampel H, Buchanan D, Arnold S, Young J, Walsh MD, Jass J, Macrae F, Antill Y, Winship IM, Giles GG, Goldblatt J, Parry S, Suthers G, Leggett B, Butz M, Aronson M, Poynter JN, Baron JA, Le Marchand L, Haile R, Gallinger S, Hopper JL, Potter J, de la Chapelle A, Vasen HF, Dunlop MG, Thibodeau SN, Jenkins MA, Dutch Lynch Syndrome Study Group Risks of Lynch syndrome cancers for MSH6 mutation carriers. J Natl Cancer Inst. 2010;102:193–201. - PMC - PubMed
-
- Senter L, Clendenning M, Sotamaa K, Hampel H, Green J, Potter JD, Lindblom A, Lagerstedt K, Thibodeau SN, Lindor NM, Young J, Winship I, Dowty JG, White DM, Hopper JL, Baglietto L, Jenkins MA, de la Chapelle A. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology. 2008;135:419–28. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous