

Using endobronchial ultrasound features to predict lymph node metastasis in patients with lung cancer
- PMID: 21636663
- PMCID: PMC3231960
- DOI: 10.1378/chest.11-0252
Using endobronchial ultrasound features to predict lymph node metastasis in patients with lung cancer
Abstract
Purposes: Reliable staging of the mediastinum determines TNM classification and directs therapy for non-small cell lung cancer (NSCLC). Our aim was to evaluate predictors of mediastinal lymph node metastasis in patients undergoing endobronchial ultrasound (EBUS).
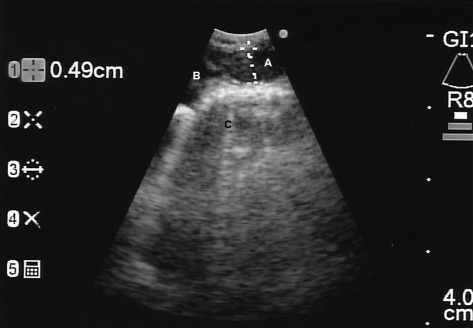
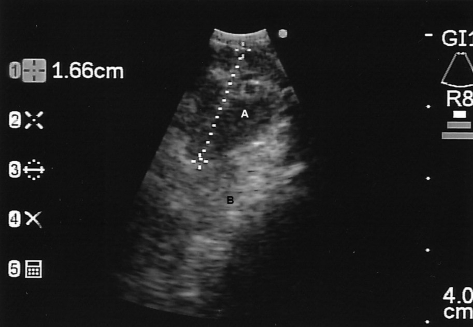
Methods: Patients with known or suspected lung cancer undergoing EBUS for staging were included. Lymph node radiographic characteristics on chest CT/PET scan and ultrasound characteristics of size, shape, border, echogenicity, and number were correlated with rapid on-site evaluation (ROSE) and final pathology. Logistic regression (estimated with generalized estimating equations to account for correlation across nodes within patients) was used with cancer (vs normal pathology) as the outcome. ORs compare risks across groups, and testing was performed with two-sided α of 0.05.
Results: Two hundred twenty-seven distinct lymph nodes (22.5% positive for malignancy) were evaluated in 100 patients. Lymph node size, by CT scan and EBUS measurements, and round and oval shape were predictive of mediastinal metastasis. Increasing size of lymph nodes on EBUS was associated with increasing malignancy risk (P = .0002). When adjusted for CT scan size, hypermetabolic lymph nodes on PET scan did not predict malignancy. Echogenicity and border contour on EBUS and site of biopsy were not significantly associated with cancer. In 94.8% of lymph nodes with a clear diagnosis, the ROSE of the first pass correlated with subsequent passes.
Conclusions: Lymph node size on CT scan and EBUS and round or oval shape by EBUS are predictors of malignancy, but no single characteristic can exclude a visualized lymph node from biopsy. Further, increasing the number of samples taken is unlikely to significantly improve sensitivity.
Figures
Comment in
-
Endobronchial ultrasound-guided biopsy of mediastinal and hilar lymph nodes: a word on false positives.Chest. 2012 Nov;142(5):1355. doi: 10.1378/chest.12-1494. Chest. 2012. PMID: 23131952 No abstract available.
References
-
- Detterbeck FC, Jantz MA, Wallace M, Vansteenkiste J, Silvestri GA, American College of Chest Physicians Invasive mediastinal staging of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132(suppl 3):202S–220S. - PubMed
-
- Silvestri GA, Gould MK, Margolis ML, et al. American College of Chest Physicians Noninvasive staging of non-small cell lung cancer: ACCP evidenced-based clinical practice guidelines (2nd edition) Chest. 2007;132(suppl 3):178S–201S. - PubMed
-
- Herth FJ, Eberhardt R. Actual role of endobronchial ultrasound (EBUS) Eur Radiol. 2007;17(7):1806–1812. - PubMed
-
- Vincent BD, El-Bayoumi E, Hoffman B, et al. Real-time endobronchial ultrasound-guided transbronchial lymph node aspiration. Ann Thorac Surg. 2008;85(1):224–230. - PubMed
-
- Wallace MB, Pascual JM, Raimondo M, et al. Minimally invasive endoscopic staging of suspected lung cancer. JAMA. 2008;299(5):540–546. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
