

Treatment of young children with localized medulloblastoma by chemotherapy alone: results of the prospective, multicenter trial HIT 2000 confirming the prognostic impact of histology
- PMID: 21636711
- PMCID: PMC3107096
- DOI: 10.1093/neuonc/nor025
Treatment of young children with localized medulloblastoma by chemotherapy alone: results of the prospective, multicenter trial HIT 2000 confirming the prognostic impact of histology
Abstract
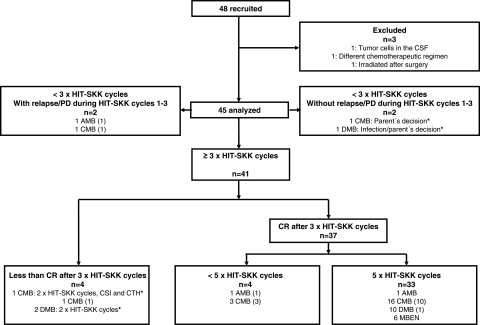
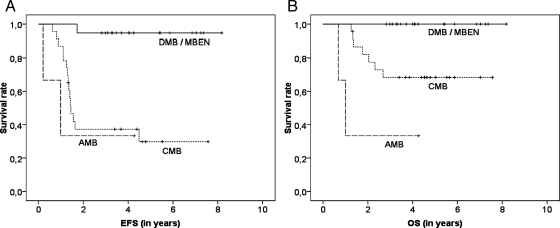
This study was designed to confirm the previously observed favorable survival rates and prognostic factors in young children with nonmetastatic medulloblastoma (MB) treated with postoperative chemotherapy alone. Patients who received a diagnosis during the period January 2001 through December 2005 and who were aged <4 years received 3 cycles of postoperative systemic multiagent chemotherapy and intraventricular methotrexate. In cases of complete remission, treatment was terminated after 2 additional cycles of chemotherapy. Otherwise, secondary surgery, radiotherapy, and consolidation chemotherapy were recommended. At a median follow-up of 4.5 years, the 5-year event-free survival (EFS) and overall survival (OS) rates (± standard error) for 45 patients (median age, 2.5 years) were 57% ± 8% and 80% ± 6%, respectively. Nineteen patients with desmoplastic/nodular MB variants had better 5-year EFS and OS rates (90% ± 7% and 100% ± 0%, respectively) than did 23 patients with classic MB (30% ± 11% and 68% ± 10%, respectively; P < .001 for EFS; P = .008 for OS). Five-year EFS and OS rates for 3 children with anaplastic MB were 33% ± 27%. Desmoplastic/nodular histology was an independent prognostic factor for EFS. Twenty-nine of 30 patients without postoperative residual tumor remained in continuous complete remission. Our results confirm that histology of MB variants is a strong prognostic factor in this age group. Sustained tumor control can be achieved by this chemotherapy regimen in young children with desmoplastic/nodular MB variants. For children with non-desmoplastic/nonnodular MB variants, for which predominantly local relapses lead to less favorable survival rates, local radiotherapy has been introduced after chemotherapy since 2006.
Figures



References
-
- Kaatsch P, Rickert CH, Kuhl J, Schuz J, Michaelis J. Population-based epidemiologic data on brain tumors in German children. Cancer. 2001;92:3155–3164. doi:10.1002/1097-0142(20011215)92:12<3155::AID-CNCR10158>3.0.CO;2-C. - DOI - PubMed
-
- Rutkowski S. Current treatment approaches to early childhood medulloblastoma. Expert Rev Neurother. 2006;6:1211–1221. doi:10.1586/14737175.6.8.1211. - DOI - PubMed
-
- Kellie SJ. Chemotherapy of central nervous system tumours in infants. Childs Nerv Syst. 1999;15:592–612. doi:10.1007/s003810050548. - DOI - PubMed
-
- Zeltzer PM, Boyett JM, Finlay JL, et al. Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: conclusions from the Children's Cancer Group 921 randomized phase III study. J Clin Oncol. 1999;17:832–845. - PubMed
-
- Packer RJ, Rood BR, MacDonald TJ. Medulloblastoma: present concepts of stratification into risk groups. Pediatr Neurosurg. 2003;39:60–67. doi:10.1159/000071316. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
