

Intermittent versus continuous oxaliplatin and fluoropyrimidine combination chemotherapy for first-line treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial
- PMID: 21641867
- PMCID: PMC3159416
- DOI: 10.1016/S1470-2045(11)70102-4
Intermittent versus continuous oxaliplatin and fluoropyrimidine combination chemotherapy for first-line treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial
Abstract
Background: When cure is impossible, cancer treatment should focus on both length and quality of life. Maximisation of time without toxic effects could be one effective strategy to achieve both of these goals. The COIN trial assessed preplanned treatment holidays in advanced colorectal cancer to achieve this aim.
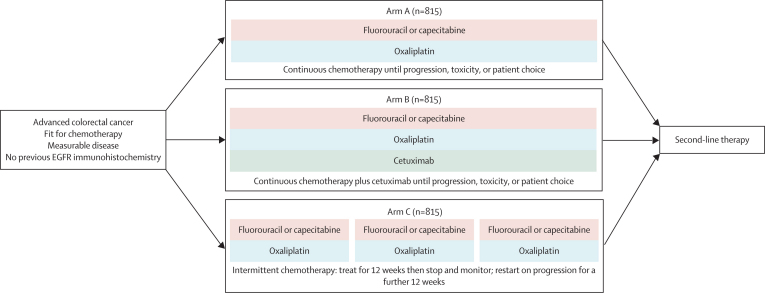
Methods: COIN was a randomised controlled trial in patients with previously untreated advanced colorectal cancer. Patients received either continuous oxaliplatin and fluoropyrimidine combination (arm A), continuous chemotherapy plus cetuximab (arm B), or intermittent (arm C) chemotherapy. In arms A and B, treatment continued until development of progressive disease, cumulative toxic effects, or the patient chose to stop. In arm C, patients who had not progressed at their 12-week scan started a chemotherapy-free interval until evidence of disease progression, when the same treatment was restarted. Randomisation was done centrally (via telephone) by the MRC Clinical Trials Unit using minimisation. Treatment allocation was not masked. The comparison of arms A and B is described in a companion paper. Here, we compare arms A and C, with the primary objective of establishing whether overall survival on intermittent therapy was non-inferior to that on continuous therapy, with a predefined non-inferiority boundary of 1.162. Intention-to-treat (ITT) and per-protocol analyses were done. This trial is registered, ISRCTN27286448.
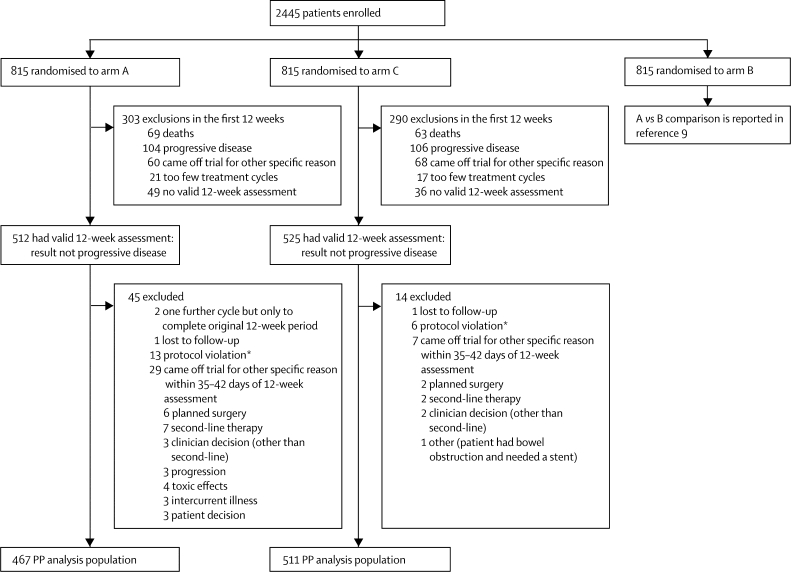
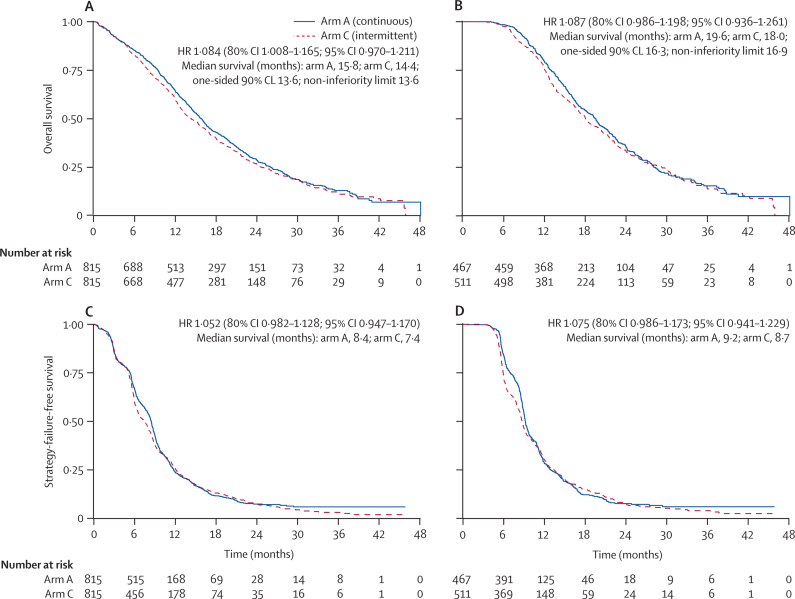
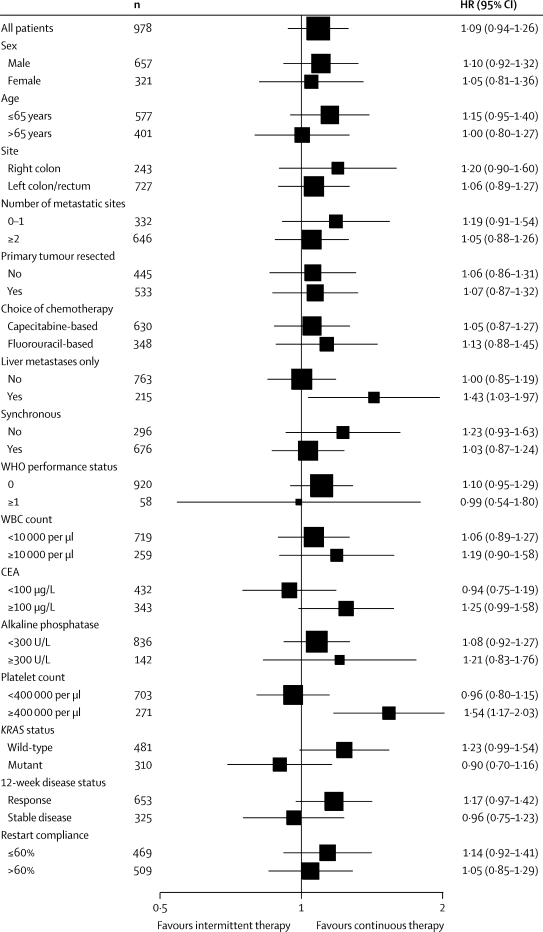
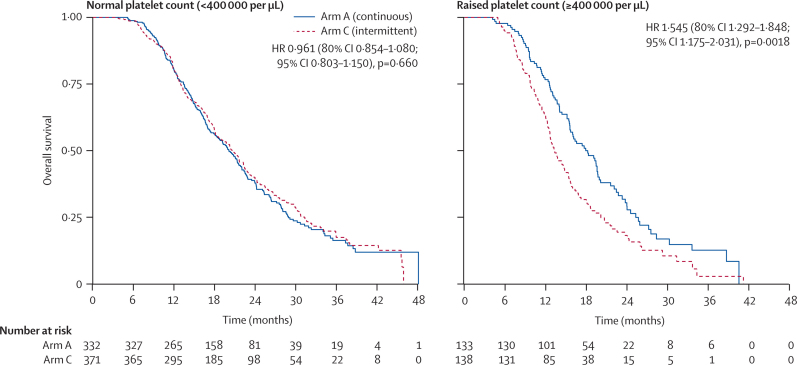
Findings: 1630 patients were randomly assigned to treatment groups (815 to continuous and 815 to intermittent therapy). Median survival in the ITT population (n=815 in both groups) was 15.8 months (IQR 9.4-26.1) in arm A and 14.4 months (8.0-24.7) in arm C (hazard ratio [HR] 1.084, 80% CI 1.008-1.165). In the per-protocol population (arm A, n=467; arm C, n=511), median survival was 19.6 months (13.0-28.1) in arm A and 18.0 months (12.1-29.3) in arm C (HR 1.087, 0.986-1.198). The upper limits of CIs for HRs in both analyses were greater than the predefined non-inferiority boundary. Preplanned subgroup analyses in the per-protocol population showed that a raised baseline platelet count, defined as 400,000 per μL or higher (271 [28%] of 978 patients), was associated with poor survival with intermittent chemotherapy: the HR for comparison of arm C and arm A in patients with a normal platelet count was 0.96 (95% CI 0.80-1.15, p=0.66), versus 1.54 (1.17-2.03, p=0.0018) in patients with a raised platelet count (p=0.0027 for interaction). In the per-protocol population, more patients on continuous than on intermittent treatment had grade 3 or worse haematological toxic effects (72 [15%] vs 60 [12%]), whereas nausea and vomiting were more common on intermittent treatment (11 [2%] vs 43 [8%]). Grade 3 or worse peripheral neuropathy (126 [27%] vs 25 [5%]) and hand-foot syndrome (21 [4%] vs 15 [3%]) were more frequent on continuous than on intermittent treatment.
Interpretation: Although this trial did not show non-inferiority of intermittent compared with continuous chemotherapy for advanced colorectal cancer in terms of overall survival, chemotherapy-free intervals remain a treatment option for some patients with advanced colorectal cancer, offering reduced time on chemotherapy, reduced cumulative toxic effects, and improved quality of life. Subgroup analyses suggest that patients with normal baseline platelet counts could gain the benefits of intermittent chemotherapy without detriment in survival, whereas those with raised baseline platelet counts have impaired survival and quality of life with intermittent chemotherapy and should not receive a treatment break.
Funding: Cancer Research UK.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Chemotherapy: Have a break.Nat Rev Clin Oncol. 2011 Jun 28;8(8):448. doi: 10.1038/nrclinonc.2011.98. Nat Rev Clin Oncol. 2011. PMID: 21709694 No abstract available.
References
-
- Seymour MT, Maughan TS, Ledermann JA, for the FOCUS Trial Investigators and the National Cancer Research Institute Colorectal Clinical Studies Group Different strategies of sequential and combination chemotherapy for patients with poor prognosis advanced colorectal cancer (MRC FOCUS): a randomised controlled trial. Lancet. 2007;370:143–152. - PubMed
-
- Beex L, Rose C, Mouridsen H. Continuous versus intermittent tamoxifen versus intermittent/alternated tamoxifen and medroxyprogesterone acetate as first line endocrine treatment in advanced breast cancer: an EORTC phase III study (10863) Eur J Cancer. 2006;42:3178–3185. - PubMed
-
- Gennari A, Amadori D, De Lena M. Lack of benefit of maintenance paclitaxel in first-line chemotherapy in metastatic breast cancer. J Clin Oncol. 2006;24:3912–3918. - PubMed
-
- Rashid MH, Chaudhary UB. Intermittent androgen deprivation therapy for prostate cancer. Oncologist. 2004;9:295–301. - PubMed
-
- Maughan TS, James RD, Kerr DJ, on behalf of the Medical Research Council Colorectal Cancer Group Comparison of intermittent and continuous palliative chemotherapy for advanced colorectal cancer: a multicentre randomised trial. Lancet. 2003;361:457–464. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
