

KIT as a therapeutic target in metastatic melanoma
- PMID: 21642685
- PMCID: PMC3986039
- DOI: 10.1001/jama.2011.746
KIT as a therapeutic target in metastatic melanoma
Abstract
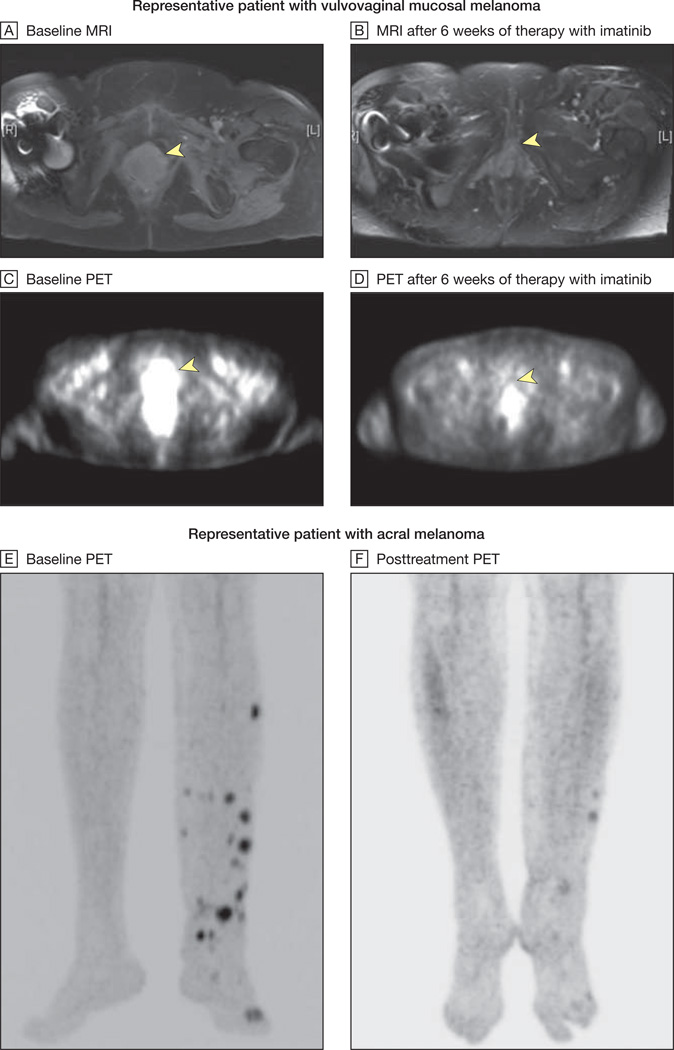
Context: Some melanomas arising from acral, mucosal, and chronically sun-damaged sites harbor activating mutations and amplification of the type III transmembrane receptor tyrosine kinase KIT. We explored the effects of KIT inhibition using imatinib mesylate in this molecular subset of disease.
Objective: To assess clinical effects of imatinib mesylate in patients with melanoma harboring KIT alterations.
Design, setting, and patients: A single-group, open-label, phase 2 trial at 1 community and 5 academic oncology centers in the United States of 295 patients with melanoma screened for the presence of KIT mutations and amplification between April 23, 2007, and April 16, 2010. A total of 51 cases with such alterations were identified and 28 of these patients were treated who had advanced unresectable melanoma arising from acral, mucosal, and chronically sun-damaged sites.
Intervention: Imatinib mesylate, 400 mg orally twice daily.
Main outcome measures: Radiographic response, with secondary end points including time to progression, overall survival, and correlation of molecular alterations and clinical response.
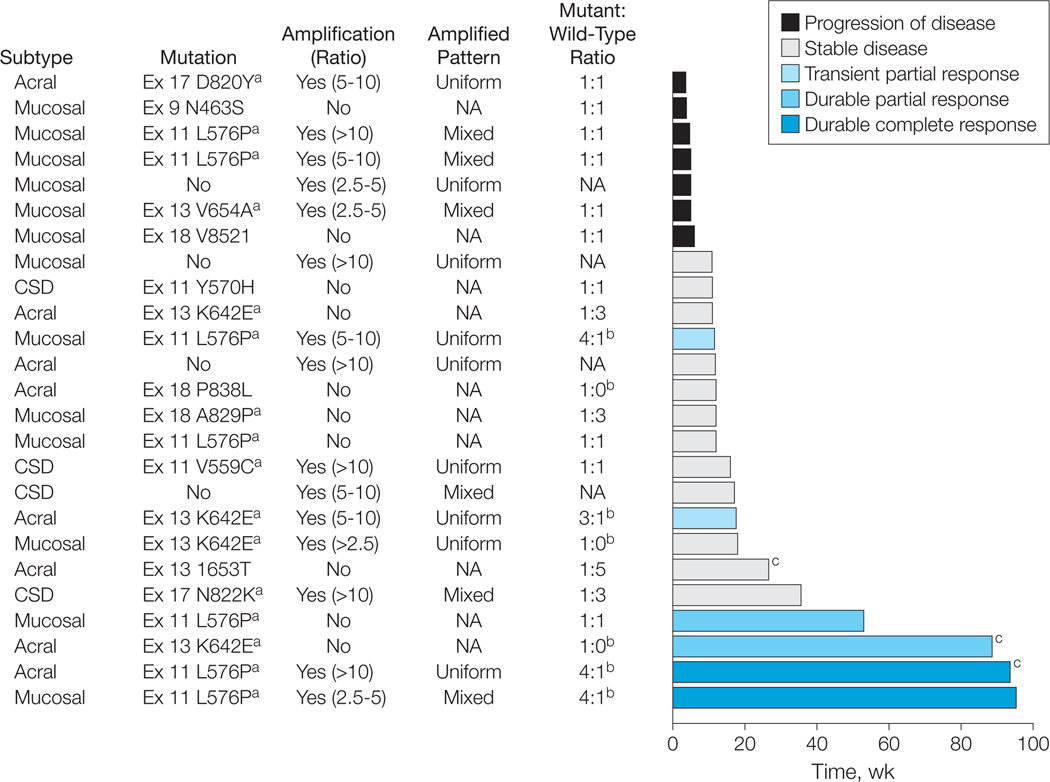
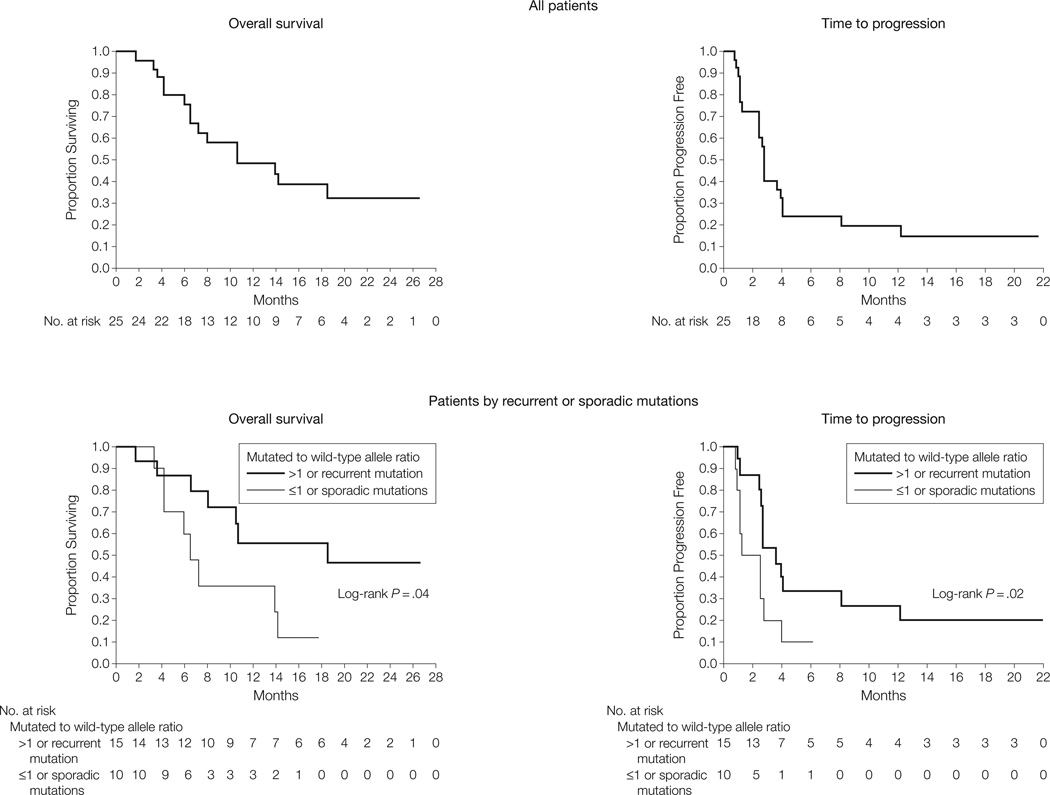
Results: Two complete responses lasting 94 (ongoing) and 95 weeks, 2 durable partial responses lasting 53 and 89 (ongoing) weeks, and 2 transient partial responses lasting 12 and 18 weeks among the 25 evaluable patients were observed. The overall durable response rate was 16% (95% confidence interval [CI], 2%-30%), with a median time to progression of 12 weeks (interquartile range [IQR], 6-18 weeks; 95% CI, 11-18 weeks), and a median overall survival of 46.3 weeks (IQR, 28 weeks-not achieved; 95% CI, 28 weeks-not achieved). Response rate was better in cases with mutations affecting recurrent hotspots or with a mutant to wild-type allelic ratio of more than 1 (40% vs 0%, P = .05), indicating positive selection for the mutated allele.
Conclusions: Among patients with advanced melanoma harboring KIT alterations, treatment with imatinib mesylate results in significant clinical responses in a subset of patients. Responses may be limited to tumors harboring KIT alterations of proven functional relevance. Trial Registration clinicaltrials.gov Identifier: NCT00470470.
Conflict of interest statement
Figures
Comment in
-
Genetics: A new tool for the KIT.Nat Rev Clin Oncol. 2011 Jun 28;8(8):446. doi: 10.1038/nrclinonc.2011.97. Nat Rev Clin Oncol. 2011. PMID: 21709696 No abstract available.
References
-
- Geller AC, Miller DR, Annas GD, Demierre MF, Gilchrest BA, Koh HK. Melanoma incidence and mortality among US whites, 1969–1999. JAMA. 2002;288(14):1719–1720. - PubMed
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300. - PubMed
-
- Chapman PB, Einhorn LH, Meyers ML, et al. Phase III multicenter randomized trial of the Dartmouth regimen versus dacarbazine in patients with meta-static melanoma. J Clin Oncol. 1999;17(9):2745–2751. - PubMed
-
- Atkins MB, Lotze MT, Dutcher JP, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993. J Clin Oncol. 1999;17(7):2105–2116. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
