

Using quantile regression to investigate racial disparities in medication non-adherence
- PMID: 21645379
- PMCID: PMC3121729
- DOI: 10.1186/1471-2288-11-88
Using quantile regression to investigate racial disparities in medication non-adherence
Abstract
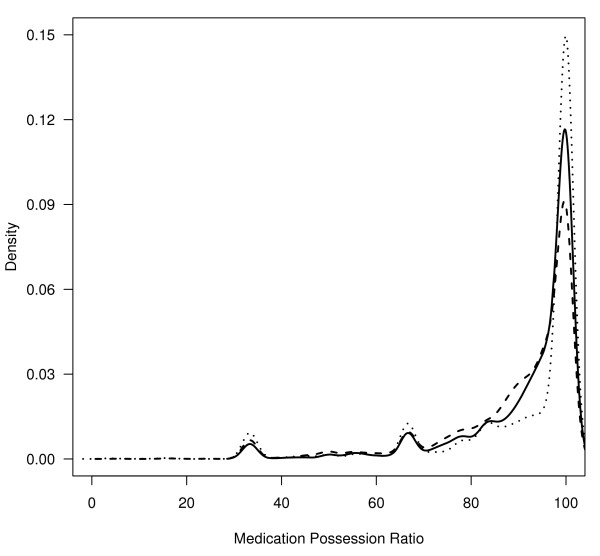
Background: Many studies have investigated racial/ethnic disparities in medication non-adherence in patients with type 2 diabetes using common measures such as medication possession ratio (MPR) or gaps between refills. All these measures including MPR are quasi-continuous and bounded and their distribution is usually skewed. Analysis of such measures using traditional regression methods that model mean changes in the dependent variable may fail to provide a full picture about differential patterns in non-adherence between groups.
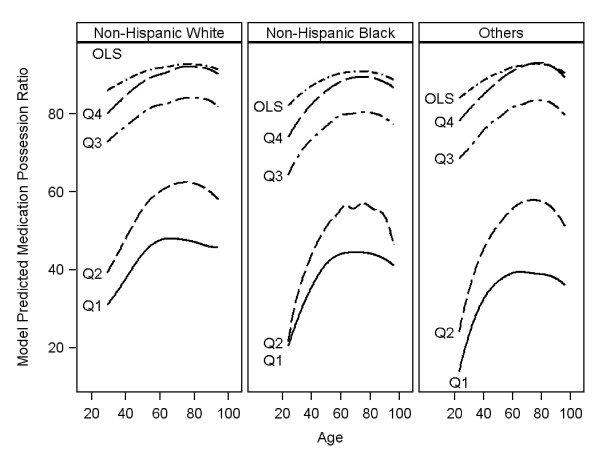
Methods: A retrospective cohort of 11,272 veterans with type 2 diabetes was assembled from Veterans Administration datasets from April 1996 to May 2006. The main outcome measure was MPR with quantile cutoffs Q1-Q4 taking values of 0.4, 0.6, 0.8 and 0.9. Quantile-regression (QReg) was used to model the association between MPR and race/ethnicity after adjusting for covariates. Comparison was made with commonly used ordinary-least-squares (OLS) and generalized linear mixed models (GLMM).
Results: Quantile-regression showed that Non-Hispanic-Black (NHB) had statistically significantly lower MPR compared to Non-Hispanic-White (NHW) holding all other variables constant across all quantiles with estimates and p-values given as -3.4% (p = 0.11), -5.4% (p = 0.01), -3.1% (p = 0.001), and -2.00% (p = 0.001) for Q1 to Q4, respectively. Other racial/ethnic groups had lower adherence than NHW only in the lowest quantile (Q1) of about -6.3% (p = 0.003). In contrast, OLS and GLMM only showed differences in mean MPR between NHB and NHW while the mean MPR difference between other racial groups and NHW was not significant.
Conclusion: Quantile regression is recommended for analysis of data that are heterogeneous such that the tails and the central location of the conditional distributions vary differently with the covariates. QReg provides a comprehensive view of the relationships between independent and dependent variables (i.e. not just centrally but also in the tails of the conditional distribution of the dependent variable). Indeed, without performing QReg at different quantiles, an investigator would have no way of assessing whether a difference in these relationships might exist.
Figures

References
-
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2008.
-
- Rozenfeld Y, Hunt JS, Plauschinat C, Wong KS. Oral antidiabetic medication adherence and glycemic control in managed care. Am J Manag Care. 2008;14(2):71–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
