

Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study
- PMID: 21645384
- PMCID: PMC3219004
- DOI: 10.1186/cc10253
Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study
Abstract
Introduction: Because of disturbed renal autoregulation, patients experiencing hypotension-induced renal insult might need higher levels of mean arterial pressure (MAP) than the 65 mmHg recommended level in order to avoid the progression of acute kidney insufficiency (AKI).
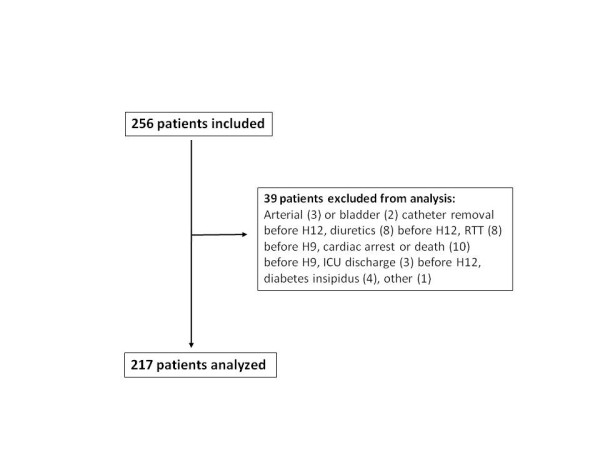
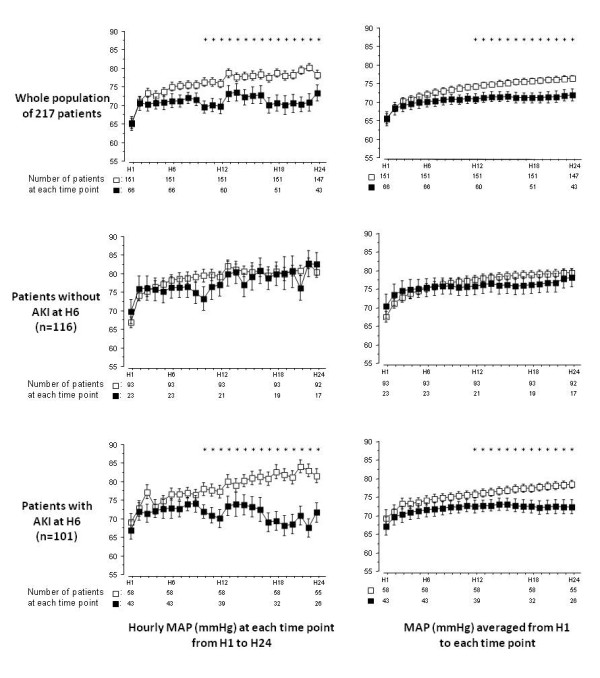
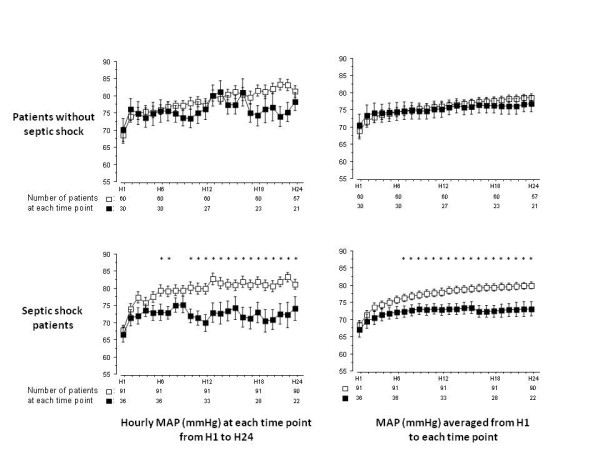
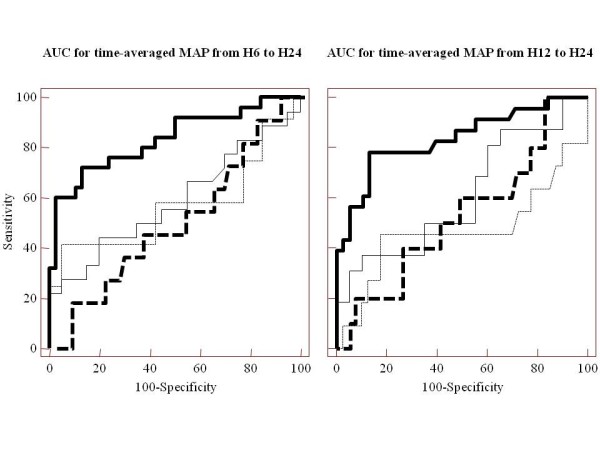
Methods: In 217 patients with sustained hypotension, enrolled and followed prospectively, we compared the evolution of the mean arterial pressure (MAP) during the first 24 hours between patients who will show AKI 72 hours after inclusion (AKIh72) and patients who will not. AKIh72 was defined as the need of renal replacement therapy or "Injury" or "Failure" classes of the 5-stage RIFLE classification (Risk, Injury, Failure, Loss of kidney function, End-stage renal disease) for acute kidney insufficiency using the creatinine and urine output criteria. This comparison was performed in four different subgroups of patients according to the presence or not of AKI at the sixth hour after inclusion (AKIh6 as defined as a serum creatinine level above 1.5 times baseline value within the first six hours) and the presence or not of septic shock at inclusion.The ability of MAP averaged over H6 to H24 to predict AKIh72 was assessed by the area under the receiver operating characteristic curve (AUC) and compared between groups.
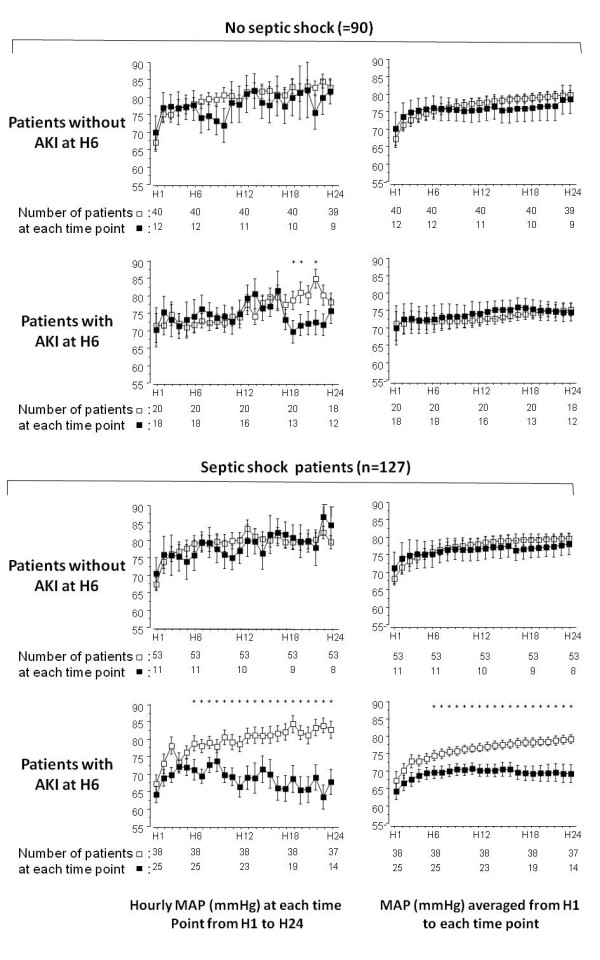
Results: The MAP averaged over H6 to H24 or over H12 to H24 was significantly lower in patients who showed AKIh72 than in those who did not, only in septic shock patients with AKIh6, whereas no link was found between MAP and AKIh72 in the three others subgroups of patients. In patients with septic shock plus AKIh6, MAP averaged over H6 to H24 or over H12 to H24 had an AUC of 0.83 (0.72 to 0.92) or 0.84 (0.72 to 0.92), respectively, to predict AKIh72 . In these patients, the best level of MAP to prevent AKIh72 was between 72 and 82 mmHg.
Conclusions: MAP about 72 to 82 mmHg could be necessary to avoid acute kidney insufficiency in patients with septic shock and initial renal function impairment.
Figures
Comment in
-
Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study.Crit Care. 2011;15(5):442. doi: 10.1186/cc10417. Epub 2011 Sep 12. Crit Care. 2011. PMID: 21939565 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
