

A comparison of dose-response characteristics of four NTCP models using outcomes of radiation-induced optic neuropathy and retinopathy
- PMID: 21645390
- PMCID: PMC3127783
- DOI: 10.1186/1748-717X-6-61
A comparison of dose-response characteristics of four NTCP models using outcomes of radiation-induced optic neuropathy and retinopathy
Abstract
Background: Biological models are used to relate the outcome of radiation therapy to dose distribution. As use of biological models in treatment planning expands, uncertainties associated with the use of specific models for predicting outcomes should be understood and quantified. In particular, the question to what extent model predictions are data-driven or dependent on the choice of the model has to be explored.
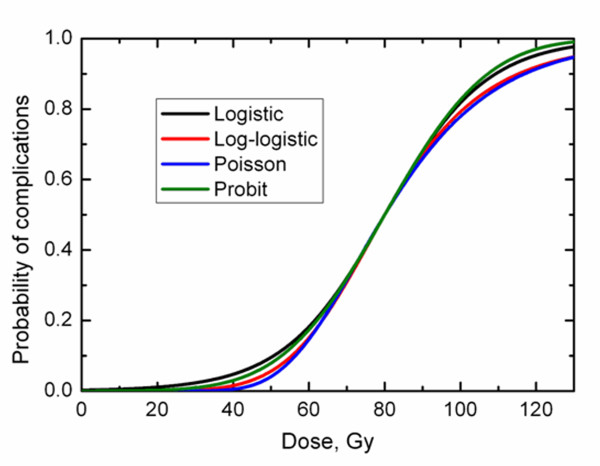
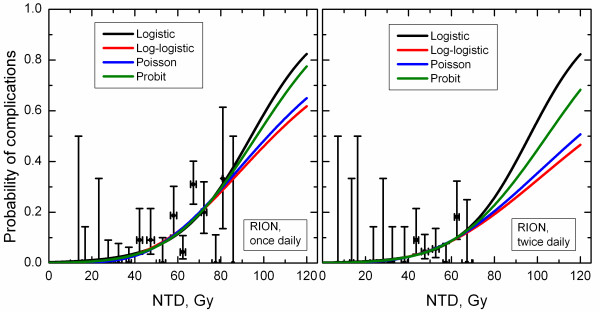
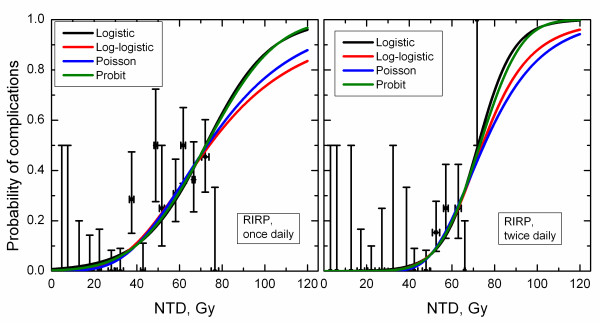
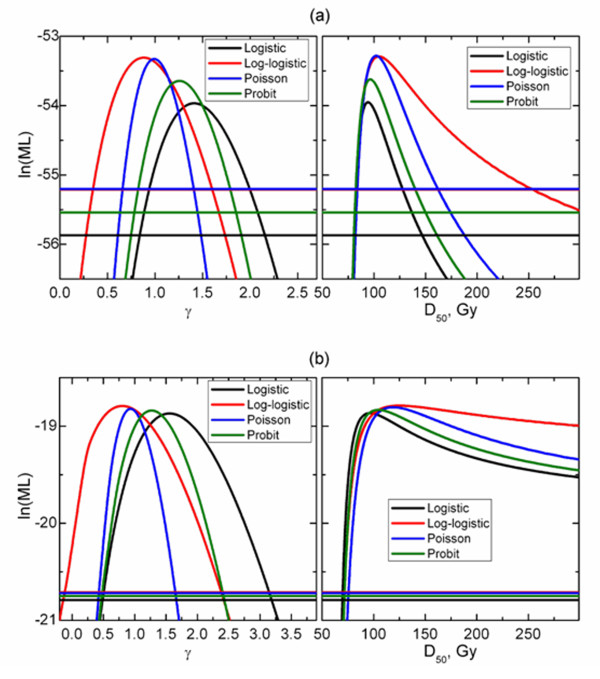
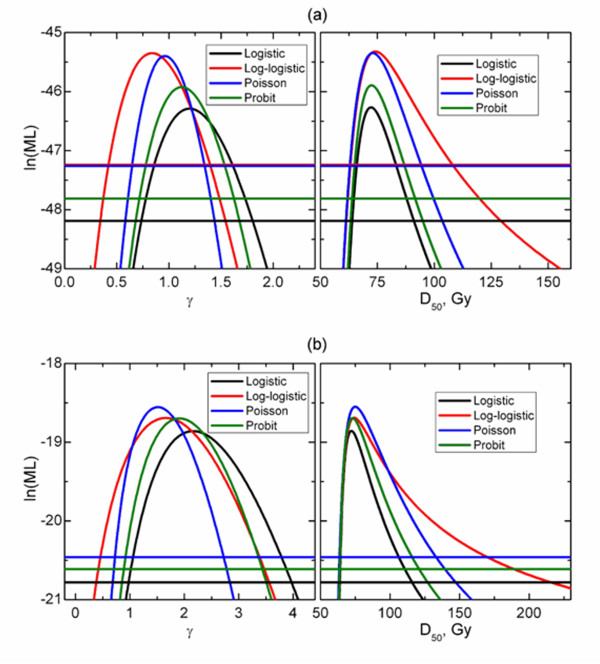
Methods: Four dose-response models--logistic, log-logistic, Poisson-based and probit--were tested for their ability and consistency in describing dose-response data for radiation-induced optic neuropathy (RION) and retinopathy (RIRP). Dose to the optic nerves was specified as the minimum dose, Dmin, received by any segment of the organ to which the damage was diagnosed by ophthalmologic evaluation. For retinopathy, the dose to the retina was specified as the highest isodose covering at least 1/3 of the retinal surface (D33%) that geometrically covered the observed retinal damage. Data on both complications were modeled separately for patients treated once daily and twice daily. Model parameters D50 and γ and corresponding confidence intervals were obtained using maximum-likelihood method.
Results: Model parameters were reasonably consistent for RION data for patients treated once daily, D50 ranging from 94.2 to 104.7 Gy and γ from 0.88 to 1.41. Similar consistency was seen for RIRP data which span a broad range of complication incidence, with D50 from 72.2 to 75.0 Gy and γ from 1.51 to 2.16 for patients treated twice daily; 72.2-74.0 Gy and 0.84-1.20 for patients treated once daily. However, large variations were observed for RION in patients treated twice daily, D50 from 96.3 to 125.2 Gy and γ from 0.80 to 1.56. Complication incidence in this dataset in any dose group did not exceed 20%.
Conclusions: For the considered data sets, the log-logistic model tends to lead to larger D50 and lower γ compared to other models for all datasets. Statements regarding normal tissue radiosensitivity and steepness of dose-response, based on model parameters, should be made with caution as the latter are not only model-dependent but also sensitive to the range of complication incidence exhibited by clinical data.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
