

Risk factors for medial meniscal pathology on knee MRI in older US adults: a multicentre prospective cohort study
- PMID: 21646417
- PMCID: PMC4864962
- DOI: 10.1136/ard.2011.150052
Risk factors for medial meniscal pathology on knee MRI in older US adults: a multicentre prospective cohort study
Abstract
Objectives: Meniscal pathology in which the aetiology is often unclear is a frequent finding on knee MRI. This study investigates potential risk factors for medial meniscal lesions or extrusion in middle-aged and elderly persons.
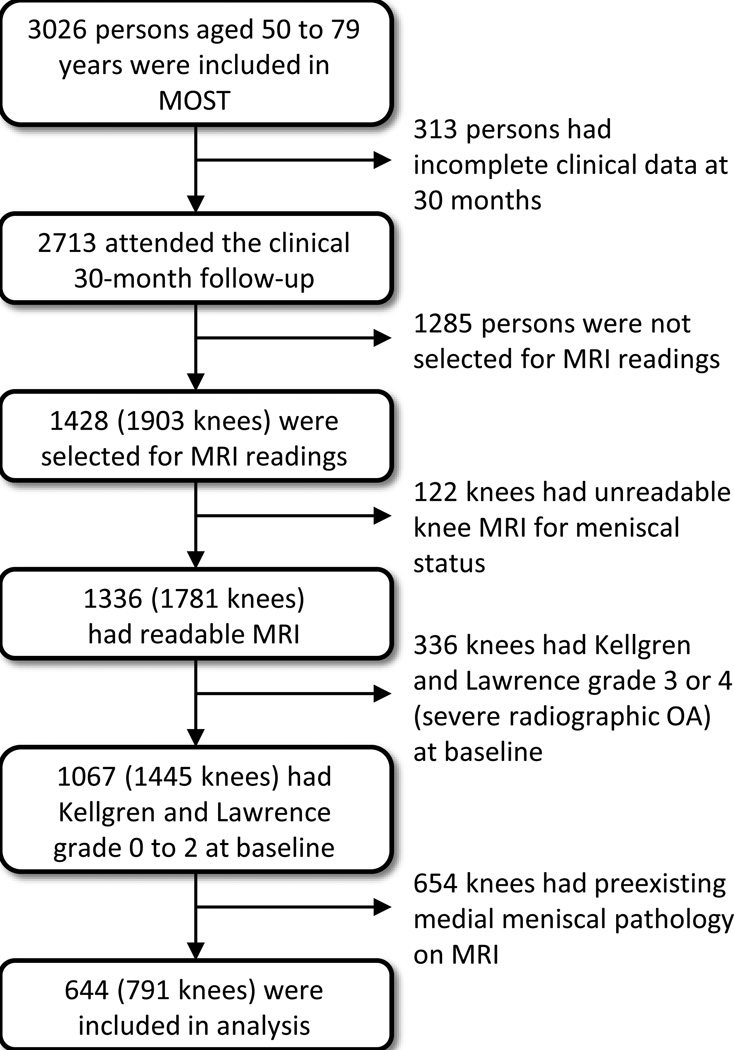
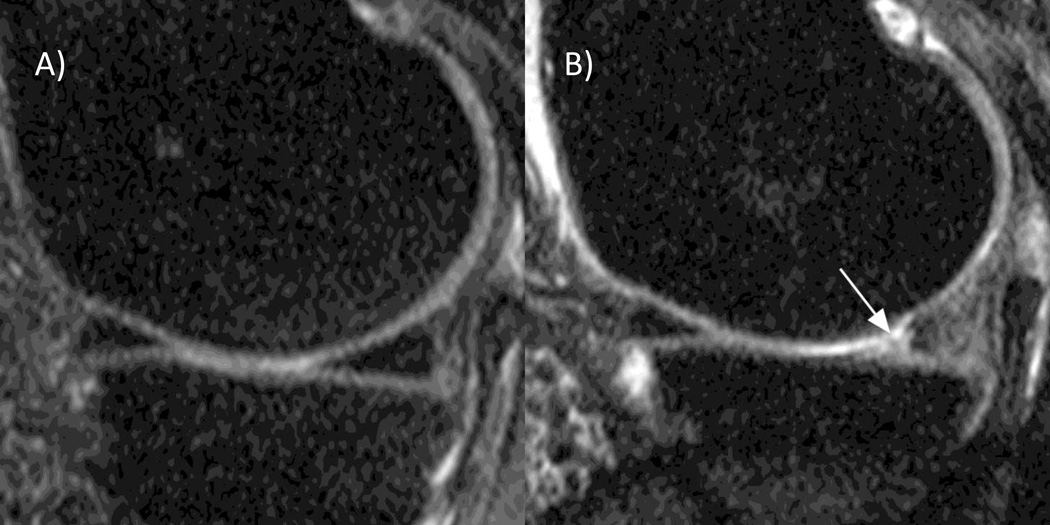
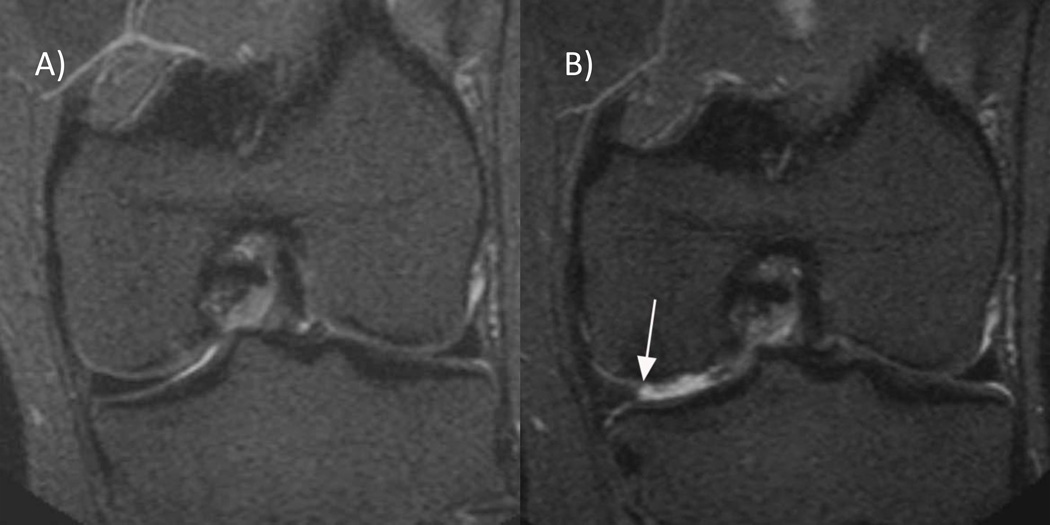
Methods: Prospective cohort study using population-based subjects from Birmingham, Alabama and Iowa City, Iowa, USA (the Multicenter Osteoarthritis Study). 644 men and women aged 50-79 years with or at high risk of knee osteoarthritis (Kellgren and Lawrence grade 0-2) but with normal medial meniscal status at baseline were studied. Paired baseline and 30-month 1.0 T knee MRI were scored for meniscal lesions and extrusion (pathology) and the following systemic, knee-specific and compartment-specific potential risk factors were evaluated: age, sex, body mass index, bony enlargement of finger joints, knee trauma, leg-length inequality and knee alignment.
Results: Of 791 knees, 77 (9.7%) had medial meniscal pathology at 30 months follow-up. 61 of the 77 (81%) had no report of trauma during follow-up. Including all potential risk factors in the multivariable model, the adjusted OR for medial meniscal pathology was 4.14 (95% CI 2.06 to 8.31) for knee trauma during follow-up, 1.64 (1.00 to 2.70) for five or more bony enlargements of finger joints (vs ≤ 4) and 2.00 (1.18 to 3.40) for varus alignment (vs not varus) at baseline examination. Obesity was a risk factor for the development of meniscal extrusion, OR 3.04 (1.04 to 8.93) but not for meniscal lesions, OR 1.15 (0.52 to 2.54).
Conclusions: Apart from knee trauma, possible generalised osteoarthritis, expressed as multiple bony enlargements of finger joints, varus alignment and obesity are risk factors for medial meniscal pathology.
Conflict of interest statement
AG is shareholder of Boston Imaging Core Lab, LLC (BICL), Boston, Massachusetts, USA, a company providing radiological image assessment services, and Synarc Inc, and consultant to Merck Serono, Novartis, Genzyme, Facet Solutions and Stryker. FWR and MDC are shareholders of BICL. None of the other authors have declared any conflict of interest.
Figures

References
-
- Fukubayashi T, Kurosawa H. The contact area and pressure distribution pattern of the knee A study of normal and osteoarthrotic knee joints. Acta Orthop Scand. 1980 Dec;51(6):871–879. - PubMed
-
- Seedhom BB, Hargreaves DJ. Transmission of the load in the knee joint with special reference to the role of the meniscus. Part I+II. Eng Med. 1979;4:207–228.
-
- Walker PS, Erkman MJ. The role of the menisci in force transmission across the knee. Clin Orthop Relat Res. 1975;(109):184–192. - PubMed
-
- Englund M, Lohmander LS. Risk factors for symptomatic knee osteoarthritis fifteen to twenty-two years after meniscectomy. Arthritis Rheum. 2004;50(9):2811–2819. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
