

Functional impairment in elderly patients with mild cognitive impairment and mild Alzheimer disease
- PMID: 21646578
- PMCID: PMC3682408
- DOI: 10.1001/archgenpsychiatry.2011.57
Functional impairment in elderly patients with mild cognitive impairment and mild Alzheimer disease
Abstract
Context: The original mild cognitive impairment (MCI) criteria exclude substantial functional deficits, but recent reports suggest otherwise. Identifying the extent, severity, type, and correlates of functional deficits that occur in MCI and mild Alzheimer disease (AD) can aid in early detection of incipient dementia and can identify potential mechanistic pathways to disrupted instrumental activities of daily living (IADLs).
Objectives: To examine the number, type, and severity of functional impairments and to identify the clinical characteristics associated with functional impairment across patients with amnestic MCI (aMCI) and those with mild AD.
Design: Study using baseline data from the Alzheimer's Disease Neuroimaging Initiative.
Setting: Multiple research sites in the United States and Canada. Patients Samples included 229 control individuals, 394 patients with aMCI, and 193 patients with AD.
Main outcome measure: The 10-item Pfeffer Functional Activities Questionnaire (FAQ) assessed function.
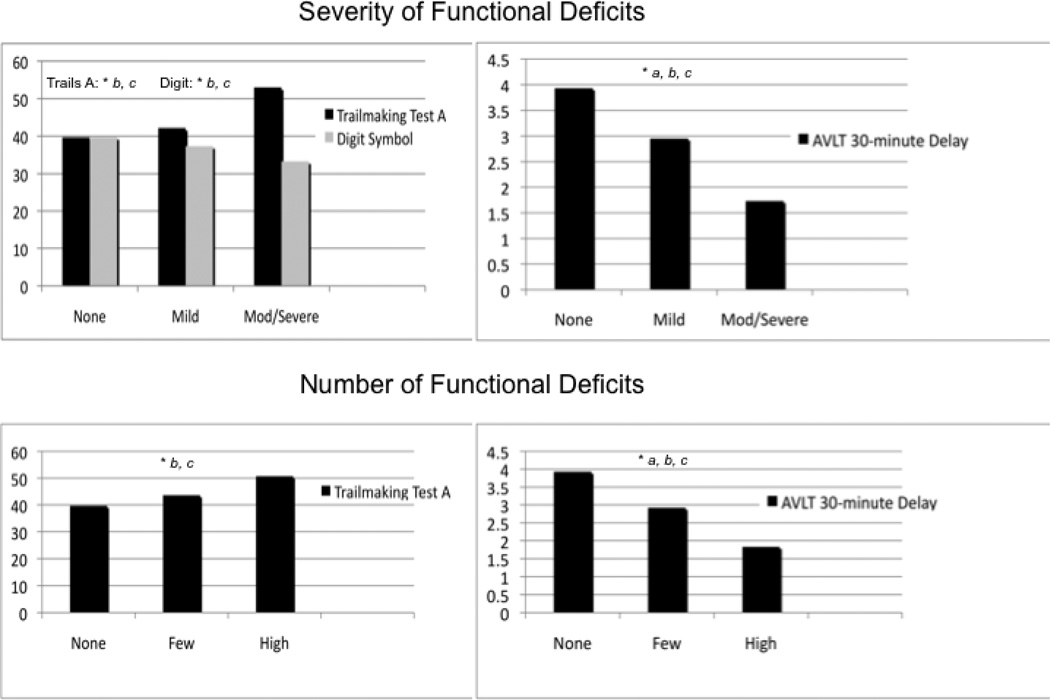
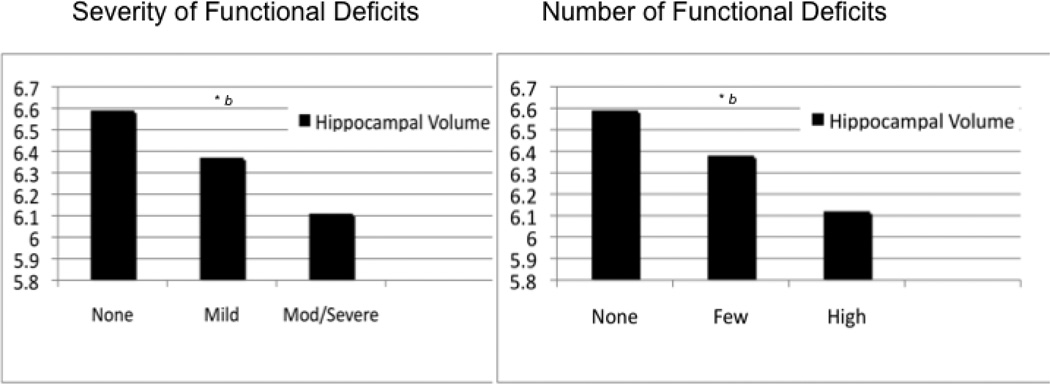
Results: Informant-reported FAQ deficits were common in patients with aMCI (72.3%) and AD (97.4%) but were rarely self-reported by controls (7.9%). The average severity per FAQ deficit did not differ between patients with aMCI and controls; both were less impaired than patients with AD (P < .001). Two FAQ items (remembering appointments, family occasions, holidays, and medications and assembling tax records, business affairs, or other papers) were specific (specificity estimate, 0.95) in differentiating the control group from the combined aMCI and AD groups (only 34.0% of patients with aMCI and 3.6% of patients with AD had no difficulty with these 2 items). The severity of FAQ deficits in the combined aMCI and AD group was associated with worse Trail Making Test, part A scores and smaller hippocampal volumes (P < .001 for both). Within the aMCI group, functionally intact individuals had greater hippocampal volumes and better Auditory Verbal Learning Test 30-minute delay and Trail Making Test, part A (P < .001 for each) scores compared with individuals with moderate or severe FAQ deficits. Patients with a high number of deficits were more likely to express the apolipoprotein ε4 allele (63.8%) compared with patients with no (46.8%) or few (48.4%) functional deficits.
Conclusions: Mild IADL deficits are common in individuals with aMCI and should be incorporated into MCI criteria. Two IADLs--remembering appointments, family occasions, holidays, and medications and assembling tax records, business affairs, or other papers--appear to be characteristic of clinically significant cognitive impairment. In patients with aMCI, impairment in memory and processing speed and greater medial temporal atrophy were associated with greater IADL deficits.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Author; 2000. text revision.
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of the Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34:939–944. - PubMed
-
- Ballard C, O’Brien JT, James I, Mynt P, Lana M, Potkins D, Reinchelt K, Lee L, Swann A, Fossey J. Quality of life for people with dementia living in residential and nursing home care: The impact of performance on activities of daily living, behavioral and psychological symptoms, language skills, and psychotropic drugs. Int Psychogeriatr. 2001;13:93–106. - PubMed
-
- Gonzalez-Salvador T, Lyketsos CG, Baker A, Hovanec L, Roques C, Brandt J, Steele C. Quality of life in dementia patients in long-term care. Int J Geriatr Psychiatry. 2000;15:181–189. - PubMed
-
- Newsom JT, Shulz R. Social support as a mediator in the relation between functional status and quality of life in older adults. Psychol Aging. 1996;11:34–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
