

Effect of aspirin dose on mortality and cardiovascular events in people with diabetes: a meta-analysis
- PMID: 21647746
- PMCID: PMC3208465
- DOI: 10.1007/s11606-011-1757-y
Effect of aspirin dose on mortality and cardiovascular events in people with diabetes: a meta-analysis
Abstract
Objectives: Pharmacologic evidence suggests adequate antiplatelet activity in diabetic patients requires >100 mg aspirin daily, yet recent trials have used ≤100 mg daily. This meta-analysis explored the relationship between aspirin dose and prevention of cardiovascular events.
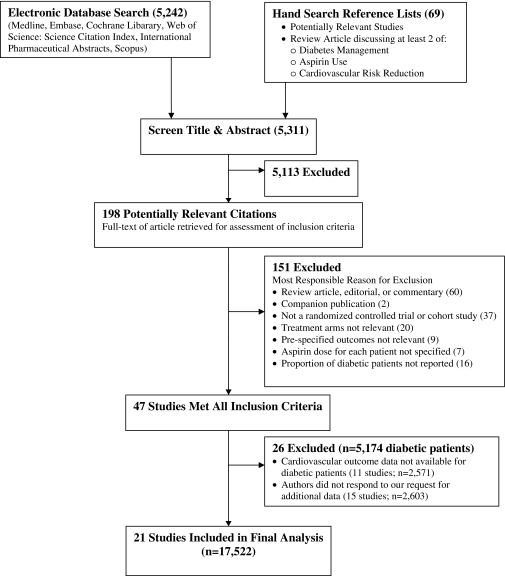
Data sources: Six electronic databases were searched using database-appropriate terms for aspirin, diabetes, and comparative study from inception until February 2010.
Review methods: Randomized controlled trials and cohort studies comparing aspirin to no antiplatelet therapy were included if they reported cardiovascular events as pre-specified outcomes, aspirin dose, and number of diabetic patients. Studies were stratified by daily aspirin dose (≤100 mg; 101-325 mg; >325 mg) and pooled risk ratios (RR) were calculated using random effects models. All-cause mortality was the primary outcome of interest. Cardiovascular-related mortality, myocardial infarction, and stroke were secondary outcomes.
Results: Data for diabetic patients were available from 21 studies (n = 17,522). Overall, 1,172 (15.4%) of 7,592 aspirin users and 1,520 (18.4%) of 8,269 controls died (p = 0.31). The pooled RRs were 0.89 (95% CI: 0.72-1.10; p = 0.27) from 13 studies using ≤100 mg (I(2) = 64%); 0.89 (95% CI: 0.61-1.30; p = 0.55) from four studies using 101-325 mg (I(2) = 83%); and 0.96 (95% CI: 0.85-1.08; p = 0.50) from eight studies using >325 mg (I(2) = 0%). Aspirin use was associated with a significantly lower risk of mortality (RR: 0.82; 95% CI: 0.69-0.98; p = 0.03) in 13 secondary prevention studies (I(2) = 27%), whereas aspirin use in seven primary prevention studies (I(2) = 0%) was not (RR: 1.01; 95% CI 0.85-1.19; p = 0.94). A substantial amount of heterogeneity was observed amongst studies in all outcomes. Although inclusion of cohort studies was a major source of heterogeneity, stratification by study design did not reveal a significant dose-response relationship.
Conclusions/interpretation: This summary of available data does not support an aspirin dose-response effect for prevention of cardiovascular events in diabetic patients. However, the systematic review identified an important gap in randomized controlled trial evidence for using 101-325 mg aspirin daily in diabetes.
References
-
- Canadian Diabetes Association Clinical Practice Guidelines Expert Committee Vascular protection in people with diabetes. Can J Diabetes. 2008;32(suppl 1):S102–S106.
-
- Ryden L, Standl E, Bartnik M, et al. Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD) Eur Heart J. 2007;28(1):88–136. doi: 10.1093/eurheartj/ehm124. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
