

The CAPRA-S score: A straightforward tool for improved prediction of outcomes after radical prostatectomy
- PMID: 21647869
- PMCID: PMC3170662
- DOI: 10.1002/cncr.26169
The CAPRA-S score: A straightforward tool for improved prediction of outcomes after radical prostatectomy
Abstract
Background: The authors previously developed and validated the Cancer of the Prostate Risk Assessment (CAPRA) score to predict prostate cancer recurrence based on pretreatment clinical data. They aimed to develop a similar postsurgical score with improved accuracy via incorporation of pathologic data.
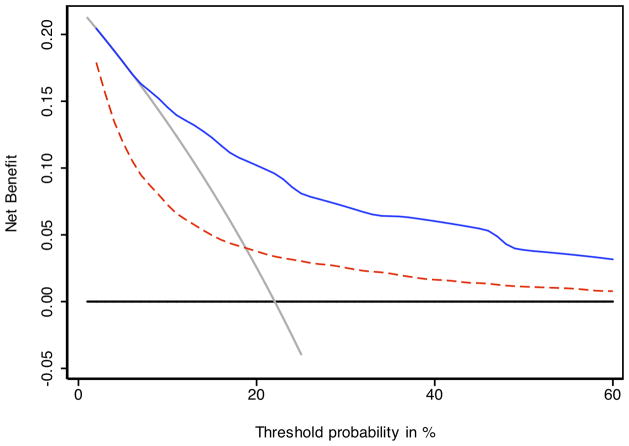
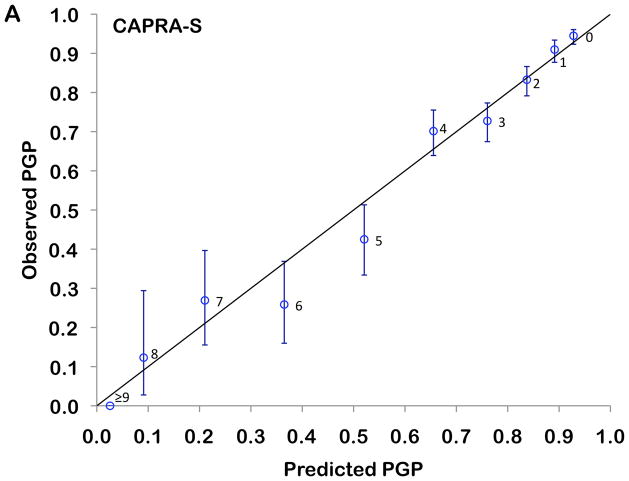
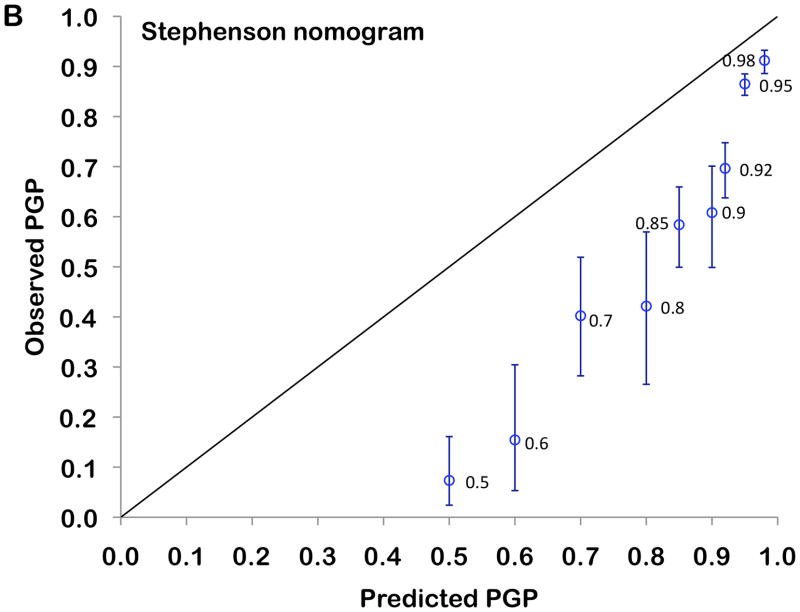
Methods: A total of 3837 prostatectomy patients in the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE™) national disease registry were analyzed. Cox regression was used to determine the predictive power of preoperative prostate-specific antigen (PSA), pathologic Gleason score (pGS), surgical margins (SM), extracapsular extension (ECE), seminal vesicle invasion (SVI), and lymph node invasion (LNI). Points were assigned based on the relative weights of these variables in predicting recurrence. The new postsurgical score (CAPRA-S) was tested and compared with a commonly cited nomogram with proportional hazards analysis, concordance (c) index, calibration plots, and decision-curve analysis.
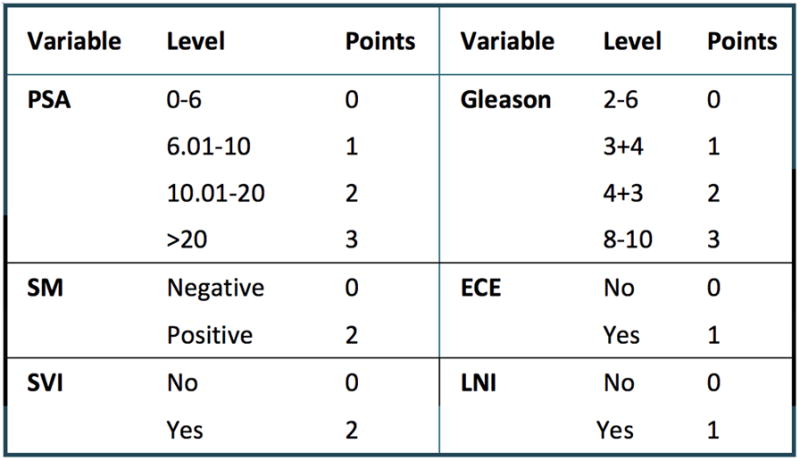
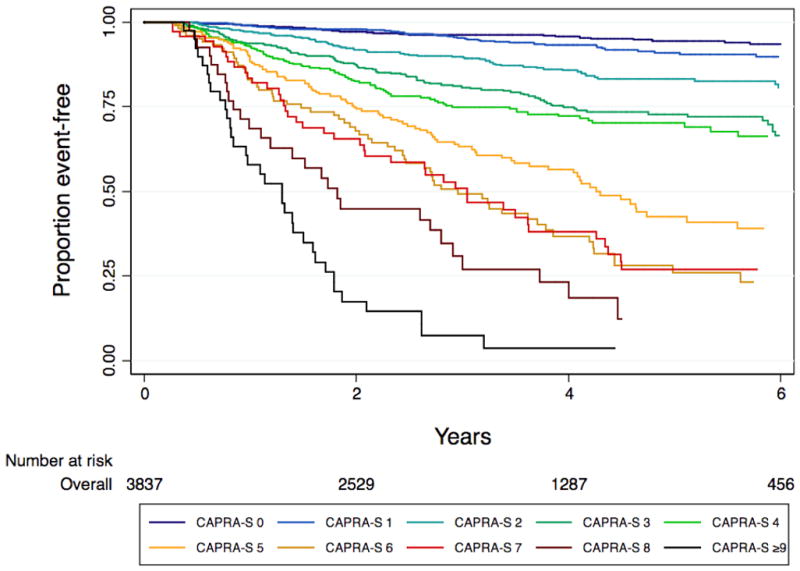
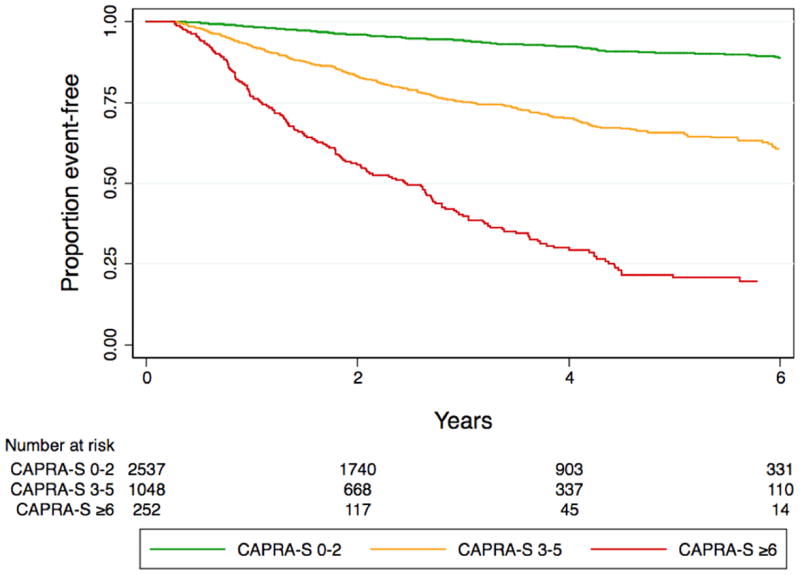
Results: Recurrence appeared in 16.8% of the men; actuarial progression-free probability at 5 years was 78.0%. The CAPRA-S was determined by adding up to 3 points for PSA, up to 3 points for pGS, 1 point each for ECE and LNI, and 2 points each for SM and SVI. The hazard ratio for each point increase in CAPRA-S score was 1.54 (95% confidence interval, 1.49-1.59), indicating a 2.4-fold increase in risk for each 2-point increase in score. The CAPRA-S c-index was 0.77, substantially higher than 0.66 for the pretreatment CAPRA score and comparable to 0.76 for the nomogram. The CAPRA-S score performed better in both calibration and decision curve analyses.
Conclusions: The CAPRA-S offers good discriminatory accuracy, calibration, and ease of calculation for clinical and research settings.
Copyright © 2011 American Cancer Society.
Figures
Comment in
-
Making and evaluating a statistical prediction model for the absolute risk of prostate cancer recurrence.Cancer. 2011 Nov 15;117(22):5026-8. doi: 10.1002/cncr.26174. Epub 2011 Jun 3. Cancer. 2011. PMID: 21647870 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Cooperberg MR, Pasta DJ, Elkin EP, Litwin MS, Latini DM, Du Chane J, et al. The University of California, San Francisco Cancer of the Prostate Risk Assessment score: a straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J Urol. 2005;173(6):1938–42. - PMC - PubMed
-
- Zhao KH, Hernandez DJ, Han M, Humphreys EB, Mangold LA, Partin AW. External validation of University of California, San Francisco, Cancer of the Prostate Risk Assessment score. Urology. 2008;72(2):396–400. - PubMed
-
- Lughezzani G, Budaus L, Isbarn H, Sun M, Perrotte P, Haese A, et al. Head-to-head comparison of the three most commonly used preoperative models for prediction of biochemical recurrence after radical prostatectomy. Eur Urol. 2010;57:562–8. - PubMed
-
- Cooperberg MR, Freedland SJ, Pasta DJ, Elkin EP, Presti JC, Jr, Amling CL, et al. Multiinstitutional validation of the UCSF cancer of the prostate risk assessment for prediction of recurrence after radical prostatectomy. Cancer. 2006;107(10):2384–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
