

HIV and chronic obstructive pulmonary disease: is it worse and why?
- PMID: 21653535
- PMCID: PMC3132792
- DOI: 10.1513/pats.201006-045WR
HIV and chronic obstructive pulmonary disease: is it worse and why?
Abstract
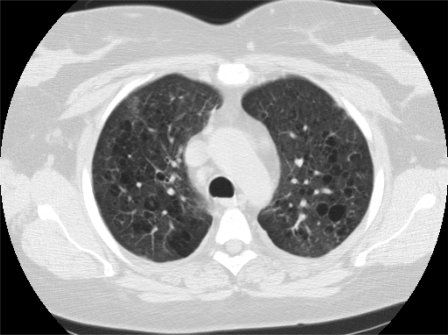
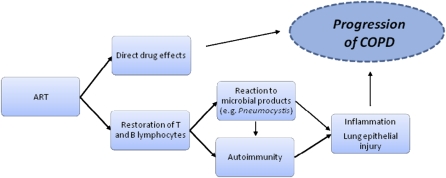
Smoking-related diseases, such as chronic obstructive pulmonary disease (COPD), are of particular concern in the HIV-infected population. Smoking rates are high in this population, and long-term exposure to cigarette smoke in the setting of HIV infection may increase the number of complications seen. Before the era of combination antiretroviral therapy, HIV-infected persons were noted to have an accelerated form of COPD, with significant emphysematous disease seen in individuals less than 40 years old. Unlike many of the AIDS-defining opportunistic infections, HIV-associated COPD may be more common in the current era of HIV because it is frequently reported in patients without a history of AIDS-related pulmonary complications and because many aging HIV-infected individuals have had a longer exposure to smoking and HIV. In this review, we document the epidemiology of HIV-associated COPD before and after the institution of combination antiretroviral therapy, review data suggesting that COPD is accelerated in those with HIV, and discuss possible mechanisms of HIV-associated COPD, including an increased susceptibility to chronic, latent infections; an aberrant inflammatory response; altered oxidant-antioxidant balance; increased apoptosis associated with HIV; and the effects of antiretroviral therapy.
Figures
References
-
- Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998;338:853–860. - PubMed
-
- (UNAIDS) Joint UN programme on HIV/AIDS. Global facts and figures. 2009.
-
- Louie JK, Hsu LC, Osmond DH, Katz MH, Schwarcz SK. Trends in causes of death among persons with acquired immunodeficiency syndrome in the era of highly active antiretroviral therapy, San Francisco, 1994–1998. J Infect Dis 2002;186:1023–1027. - PubMed
-
- Grubb JR, Moorman AC, Baker RK, Masur H. The changing spectrum of pulmonary disease in patients with HIV infection on antiretroviral therapy. AIDS 2006;20:1095–1107. - PubMed
-
- Global initiative for chronic obstructive lung disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO workshop report. Bethesda, National Heart, Lung, and Blood Institute, December 2009. Available from: wwwgoldCOPDcom.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical