

Oxidative damage in multiple sclerosis lesions
- PMID: 21653539
- PMCID: PMC3122372
- DOI: 10.1093/brain/awr128
Oxidative damage in multiple sclerosis lesions
Abstract
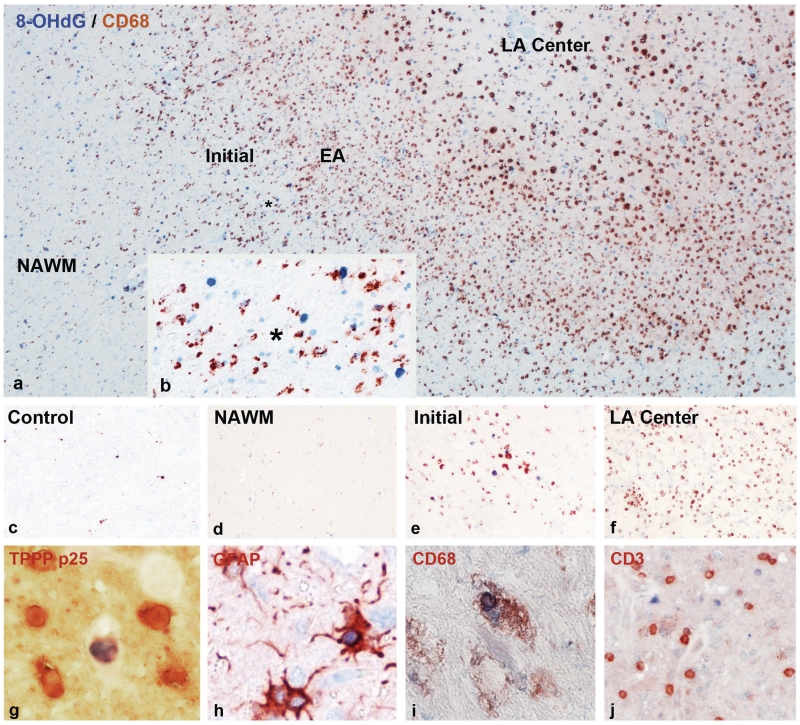
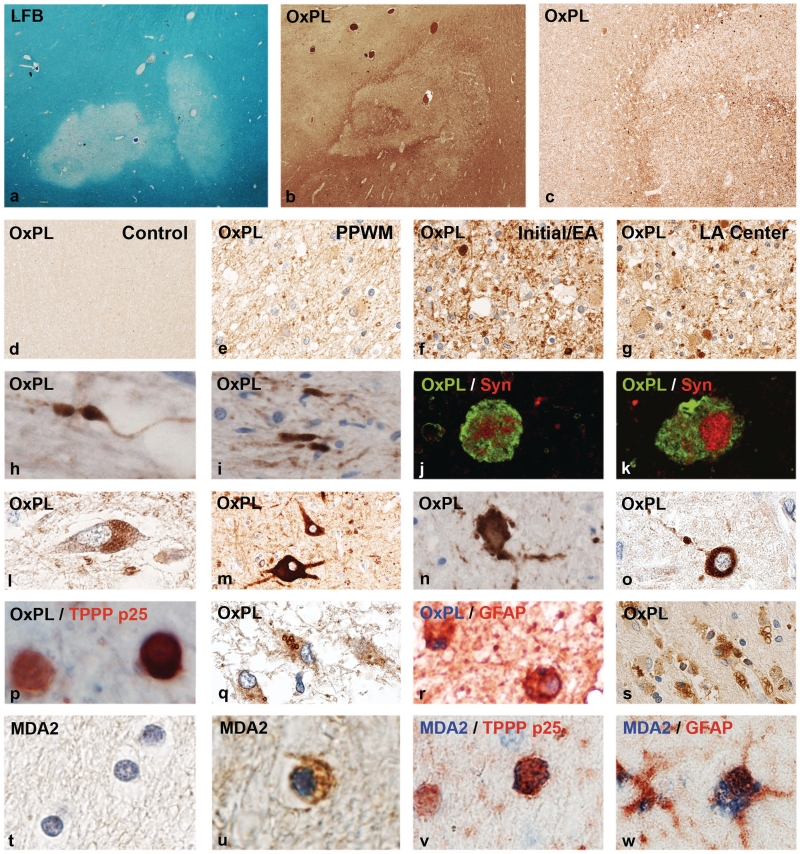
Multiple sclerosis is a chronic inflammatory disease of the central nervous system, associated with demyelination and neurodegeneration. The mechanisms of tissue injury are currently poorly understood, but recent data suggest that mitochondrial injury may play an important role in this process. Since mitochondrial injury can be triggered by reactive oxygen and nitric oxide species, we analysed by immunocytochemistry the presence and cellular location of oxidized lipids and oxidized DNA in lesions and in normal-appearing white matter of 30 patients with multiple sclerosis and 24 control patients without neurological disease or brain lesions. As reported before in biochemical studies, oxidized lipids and DNA were highly enriched in active multiple sclerosis plaques, predominantly in areas that are defined as initial or 'prephagocytic' lesions. Oxidized DNA was mainly seen in oligodendrocyte nuclei, which in part showed signs of apoptosis. In addition, a small number of reactive astrocytes revealed nuclear expression of 8-hydroxy-d-guanosine. Similarly, lipid peroxidation-derived structures (malondialdehyde and oxidized phospholipid epitopes) were seen in the cytoplasm of oligodendrocytes and some astrocytes. In addition, oxidized phospholipids were massively accumulated in a fraction of axonal spheroids with disturbed fast axonal transport as well as in neurons within grey matter lesions. Neurons stained for oxidized phospholipids frequently revealed signs of degeneration with fragmentation of their dendritic processes. The extent of lipid and DNA oxidation correlated significantly with inflammation, determined by the number of CD3 positive T cells and human leucocyte antigen-D expressing macrophages and microglia in the lesions. Our data suggest profound oxidative injury of oligodendrocytes and neurons to be associated with active demyelination and axonal or neuronal injury in multiple sclerosis.
Figures
References
-
- Aboul-Enein F, Rauschka H, Kornek B, Stadelmann C, Stefferl A, Brück W, et al. Preferential loss of myelin associated glycoprotein reflects hypoxia-like white matter damage in stroke and inflammatory brain diseases. J Neuropath Exp Neurol. 2003;62:25–33. - PubMed
-
- Barnett MH, Prineas JW. Relapsing and remitting multiple sclerosis: pathology of the newly forming lesion. Ann Neurol. 2004;55:458–68. - PubMed
-
- Bauer J, Elger CE, Hans VH, Schramm J, Urbach H, Lassmann H, et al. Astrocytes are a specific immunological target in Rasmussen's encephalitis. Ann Neurol. 2007;62:67–80. - PubMed
-
- Bizzozero OA, Dejesus G, Callaha K, Pastuszyn A. Elevated protein carbonylation in the brain white matter and grey matter of patients with multiple sclerosis. J Neurosci Res. 2005;81:687–95. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
