

A dominant mutation in RPE65 identified by whole-exome sequencing causes retinitis pigmentosa with choroidal involvement
- PMID: 21654732
- PMCID: PMC3190249
- DOI: 10.1038/ejhg.2011.86
A dominant mutation in RPE65 identified by whole-exome sequencing causes retinitis pigmentosa with choroidal involvement
Erratum in
- Eur J Hum Genet. 2011 Oct;19(10):1109
Abstract
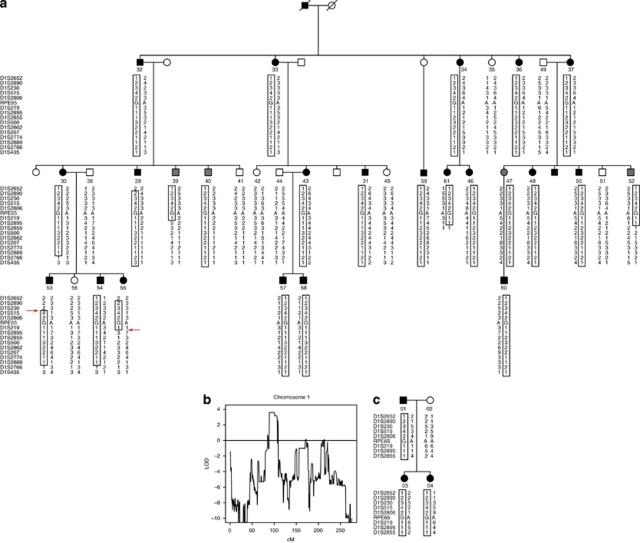
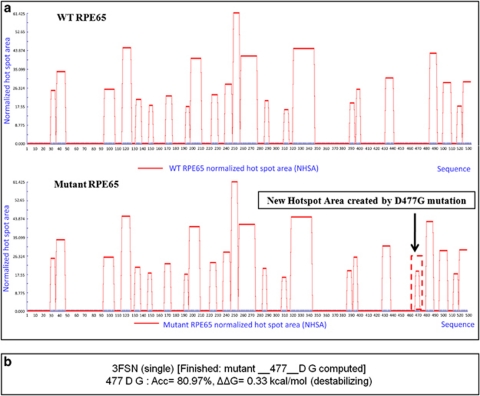
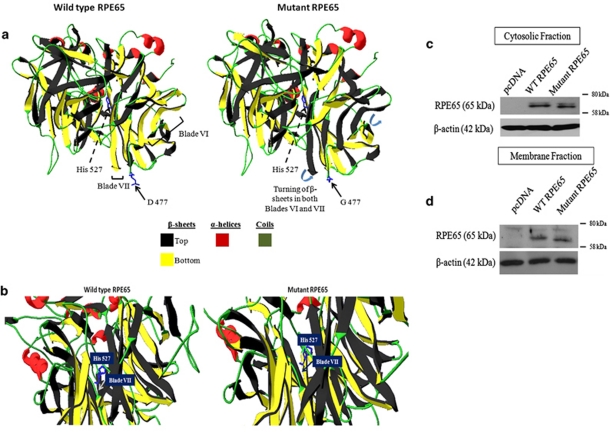
Linkage testing using Affymetrix 6.0 SNP Arrays mapped the disease locus in TCD-G, an Irish family with autosomal dominant retinitis pigmentosa (adRP), to an 8.8 Mb region on 1p31. Of 50 known genes in the region, 11 candidates, including RPE65 and PDE4B, were sequenced using di-deoxy capillary electrophoresis. Simultaneously, a subset of family members was analyzed using Agilent SureSelect All Exome capture, followed by sequencing on an Illumina GAIIx platform. Candidate gene and exome sequencing resulted in the identification of an Asp477Gly mutation in exon 13 of the RPE65 gene tracking with the disease in TCD-G. All coding exons of genes not sequenced to sufficient depth by next generation sequencing were sequenced by di-deoxy sequencing. No other potential disease-causing variants were found to segregate with disease in TCD-G. The Asp477Gly mutation was not present in Irish controls, but was found in a second Irish family provisionally diagnosed with choroideremia, bringing the combined maximum two-point LOD score to 5.3. Mutations in RPE65 are a known cause of recessive Leber congenital amaurosis (LCA) and recessive RP, but no dominant mutations have been reported. Protein modeling suggests that the Asp477Gly mutation may destabilize protein folding, and mutant RPE65 protein migrates marginally faster on SDS-PAGE, compared with wild type. Gene therapy for LCA patients with RPE65 mutations has shown great promise, raising the possibility of related therapies for dominant-acting mutations in this gene.
Figures
References
-
- Heckenlively JR. Retinitis Pigmentosa. Philadelphia, PA, USA: J.B. Lippincott; 1988.
-
- Heckenlively JR, Daiger SP.Hereditary Retinal and Choroidal Degenerations5th edn.New York, NY, USA: Churchill Livingston Elsevier; 2007
-
- Haim M. Epidemiology of retinitis pigmentosa in Denmark. Acta Ophthalmol Scand Suppl. 2002;233:1–34. - PubMed
-
- RetNet The Retinal Information Network http://www.sph.uth.tmc.edu/RetNet/ Stephen P. Daiger, PhD, Administrator, The Univ. of Texas Health Science Center at Houston,1996-present
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
