

Lipoprotein associated phospholipase A(2): role in atherosclerosis and utility as a biomarker for cardiovascular risk
- PMID: 21654904
- PMCID: PMC3084931
- DOI: 10.1007/s13167-011-0063-4
Lipoprotein associated phospholipase A(2): role in atherosclerosis and utility as a biomarker for cardiovascular risk
Abstract
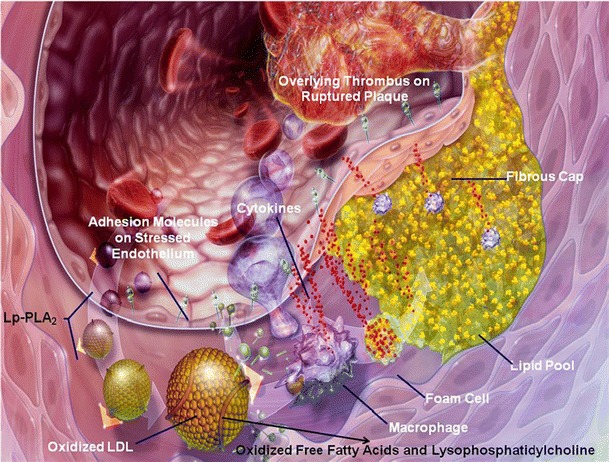
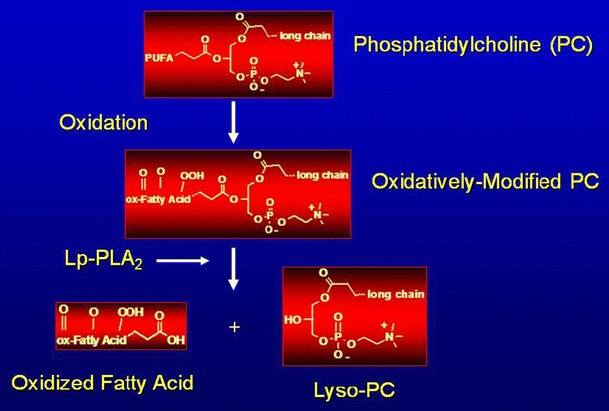
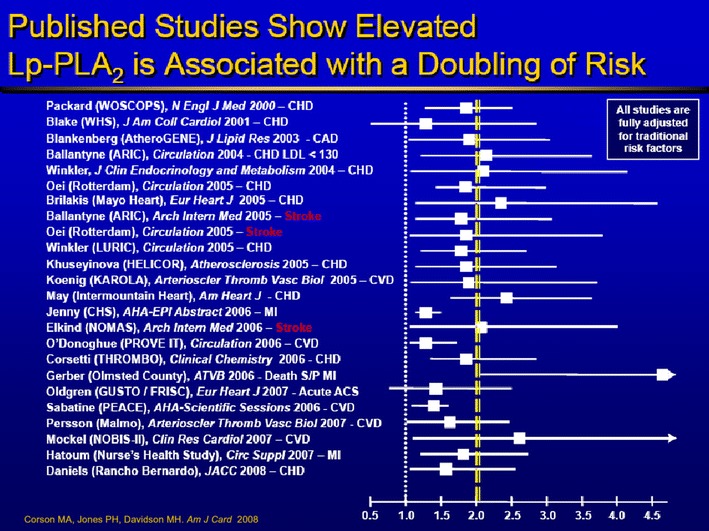
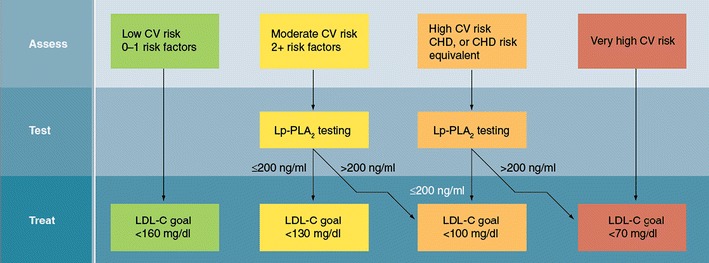
Atherosclerosis and its clinical manifestations are widely prevalent throughout the world. Atherogenesis is highly complex and modulated by numerous genetic and environmental risk factors. A large body of basic scientific and clinical research supports the conclusion that inflammation plays a significant role in atherogenesis along the entire continuum of its progression. Inflammation adversely impacts intravascular lipid handling and metabolism, resulting in the development of macrophage foam cell, fatty streak, and atheromatous plaque formation. Given the enormous human and economic cost of myocardial infarction, ischemic stroke, peripheral arterial disease and amputation, and premature death and disability, considerable effort is being committed to refining our ability to correctly identify patients at heightened risk for atherosclerotic vascular disease and acute cardiovascular events so that they can be treated earlier and more aggressively. Serum markers of inflammation have emerged as an important component of risk factor burden. Lipoprotein-associated phospholipase A2 (Lp-PLA(2)) potentiates intravascular inflammation and atherosclerosis. A variety of epidemiologic studies support the utility of Lp-PLA(2) measurements for estimating and further refining cardiovascular disease risk. Drug therapies to inhibit Lp-PLA(2) are in development and show considerable promise, including darapladib, a specific molecular inhibitor of the enzyme. In addition to substantially inhibiting Lp-PLA(2) activity, darapladib reduces progression of the necrotic core volume of human coronary artery atheromatous plaque. The growing body of evidence points to an important role and utility for Lp-PLA(2) testing in preventive and personalized clinical medicine.
Figures
References
-
- Libby P. What have we learned about the biology of atherosclerosis? The role of inflammation. Am J Cardiol. 2001;88:3J–6J. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
