

The impact of retail-sector delivery of artemether-lumefantrine on malaria treatment of children under five in Kenya: a cluster randomized controlled trial
- PMID: 21655317
- PMCID: PMC3104978
- DOI: 10.1371/journal.pmed.1000437
The impact of retail-sector delivery of artemether-lumefantrine on malaria treatment of children under five in Kenya: a cluster randomized controlled trial
Abstract
Background: It has been proposed that artemisinin-based combination therapy (ACT) be subsidised in the private sector in order to improve affordability and access. This study in western Kenya aimed to evaluate the impact of providing subsidized artemether-lumefantrine (AL) through retail providers on the coverage of prompt, effective antimalarial treatment for febrile children aged 3-59 months.
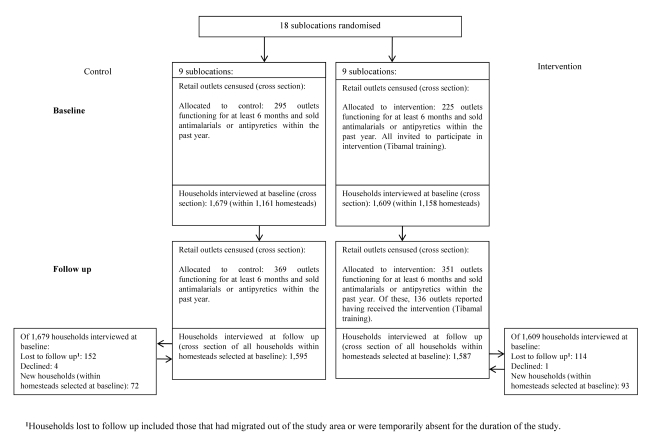
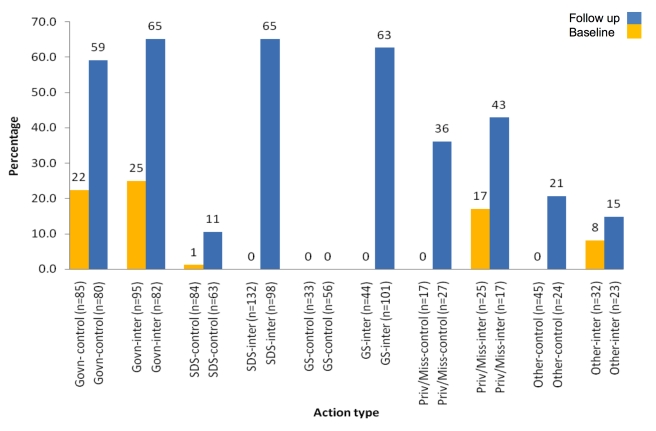
Methods and findings: We used a cluster-randomized, controlled design with nine control and nine intervention sublocations, equally distributed across three districts in western Kenya. Cross-sectional household surveys were conducted before and after the delivery of the intervention. The intervention comprised provision of subsidized packs of paediatric ACT to retail outlets, training of retail outlet staff, and community awareness activities. The primary outcome was defined as the proportion of children aged 3-59 months reporting fever in the past 2 weeks who started treatment with AL on the same day or following day of fever onset. Data were collected using structured questionnaires and analyzed based on cluster-level summaries, comparing control to intervention arms, while adjusting for other covariates. Data were collected on 2,749 children in the target age group at baseline and 2,662 at follow-up. 29% of children experienced fever within 2 weeks before the interview. At follow-up, the percentage of children receiving AL on the day of fever or the following day had risen by 14.6% points in the control arm (from 5.3% [standard deviation (SD): 3.2%] to 19.9% [SD: 10.0%]) and 40.2% points in the intervention arm (from 4.7% [SD: 3.4%] to 44.9% [SD: 11.7%]). The percentage of children receiving AL was significantly greater in the intervention arm at follow-up, with a difference between the arms of 25.0% points (95% confidence interval [CI]: 14.1%, 35.9%; unadjusted p = 0.0002, adjusted p = 0.0001). No significant differences were observed between arms in the proportion of caregivers who sought treatment for their child's fever by source, or in the child's adherence to AL.
Conclusions: Subsidizing ACT in the retail sector can significantly increase ACT coverage for reported fevers in rural areas. Further research is needed on the impact and cost-effectiveness of such subsidy programmes at a national scale.
Trial registration: Current Controlled Trials ISRCTN59275137 and Kenya Pharmacy and Poisons Board Ethical Committee for Clinical Trials PPB/ECCT/08/07.
Conflict of interest statement
RWS chairs the Novartis National Malaria Control Programme Managers "Best Practice Workshops" in Africa for which he receives an honorarium.
Figures
References
-
- World Health Organisation. 2006. Guidelines for the treatment of malaria, second edition. Available: http://www.who.int/malaria/publications/atoz/9789241547925/en/index.html. Accessed 1 May 2010.
-
- World Health Organisation. 2009. World Malaria Report. Available: http://www.who.int/malaria/world_malaria_report_2009/en/index.html. Accessed 1 May 2010.
-
- Institute of Medicine of the National Academies. Economics of Malaria Drugs in an Age of Resistance. Washington DC: National Academies Press; 2004. Saving Lives, Buying Time. - PubMed
-
- McCombie SC. Treatment seeking for malaria: a review of recent research. Soc Sci Med. 1996;43:933–945. - PubMed
-
- Williams HA, Jones CO. A critical review of behavioral issues related to malaria control in sub-Saharan Africa: what contributions have social scientists made? Soc Sci Med. 2004;59:501–523. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
