

Bariatric surgery
- PMID: 21655459
- PMCID: PMC3109275
- DOI: 10.3238/arztebl.2011.0341
Bariatric surgery
Abstract
Background: Bariatric surgery has increased in numbers, but the treatment of morbid obesity in Germany still needs improvement. The new interdisciplinary S3-guideline provides information on the appropriate indications, procedures, techniques, and follow-up care.
Methods: Systematic review of the literature, classification of the evidence, graded recommendations, and interdisciplinary consensus-building.
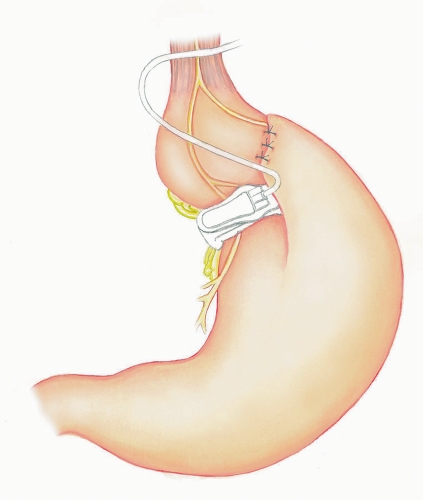
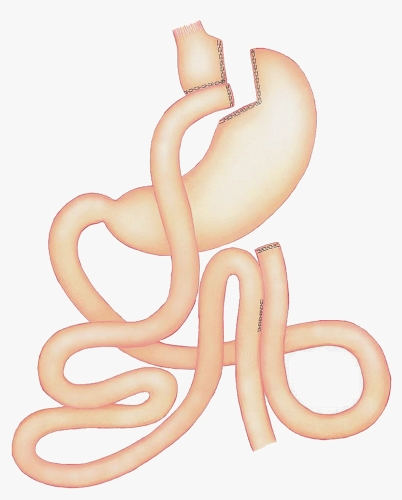
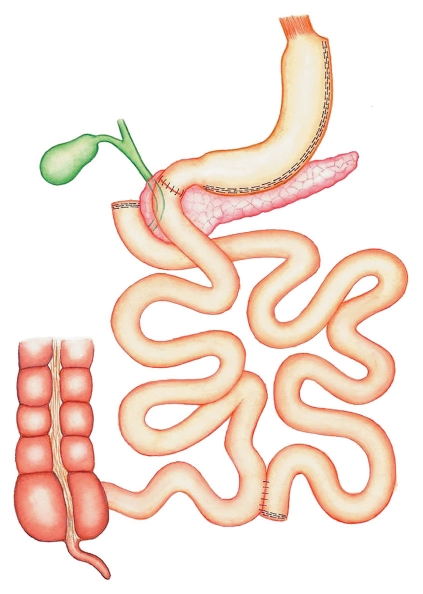
Results: Bariatric surgery is a component of the multimodal treatment of obesity, which consists of multidisciplinary evaluation and diagnosis, conservative and surgical treatments, and lifelong follow-up care. The current guideline extends the BMI-based spectrum of indications that was previously proposed (BMI greater than 40 kg/m(2), or greater than 35 kg/m(2)with secondary diseases) by eliminating age limits, as well as most of the contraindications. A prerequisite for surgery is that a structured, conservative weight-loss program has failed or is considered to be futile. Type 2 diabetes is now considered an independent indication under clinical study conditions for patients whose BMI is less than 35 kg/m(2) (metabolic surgery). The standard laparoscopic techniques are gastric banding, gastric bypass, sleeve gastrectomy, and biliopancreatic diversion. The choice of procedure is based on knowledge of the results, long-term effects, complications, and individual circumstances. Structured lifelong follow-up should be provided and should, in particular, prevent metabolic deficiencies.
Conclusion: The guideline contains recommendations based on the scientific evidence and on a consensus of experts from multiple disciplines about the indications for bariatric surgery, the choice of procedure, techniques, and follow-up care. It should be broadly implemented to improve patient care in this field.
Figures

References
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and metaanalysis. JAMA. 2004;292:1724–1737. - PubMed
-
- Buchwald H, Estok R, Fahrbach K, et al. Trends in mortality in bariatric surgery: a systematic review and meta-analysis. Surgery. 2007;142:621–632. - PubMed
-
- Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:248–256. - PubMed
-
- Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–2693. - PubMed
-
- Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–752. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical