

Myocardial ischemia induced by rapid atrial pacing causes troponin T release detectable by a highly sensitive assay: insights from a coronary sinus sampling study
- PMID: 21658559
- PMCID: PMC3130506
- DOI: 10.1016/j.jacc.2010.11.066
Myocardial ischemia induced by rapid atrial pacing causes troponin T release detectable by a highly sensitive assay: insights from a coronary sinus sampling study
Abstract
Objectives: The purpose of this study was to assess whether: 1) very small increases in troponin T, measured by a new highly sensitive cardiac troponin T (hs-cTnT), may reflect ischemia without necrosis; and 2) serial changes can discriminate ischemia from other causes of cardiac troponin T (cTnT) release.
Background: A new hs-cTnT assay offers greater sensitivity than current assays.
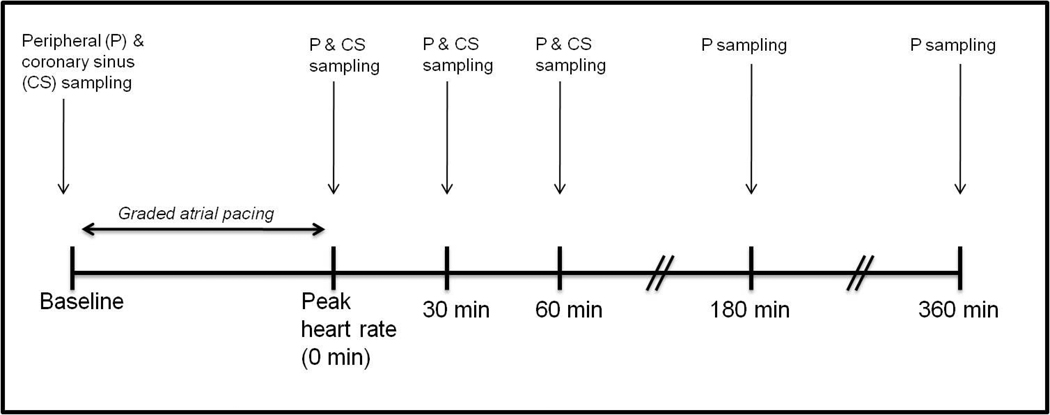
Methods: Nineteen patients referred for diagnostic catheterization underwent cannulation of the coronary sinus (CS). Serial CS and peripheral plasma samples were obtained at multiple time points during and after incremental rapid atrial pacing. cTnT was quantified using both a standard and a pre-commercial highly sensitive assay. Ischemia was determined by the presence of significant coronary artery disease (CAD) and myocardial lactate release with pacing.
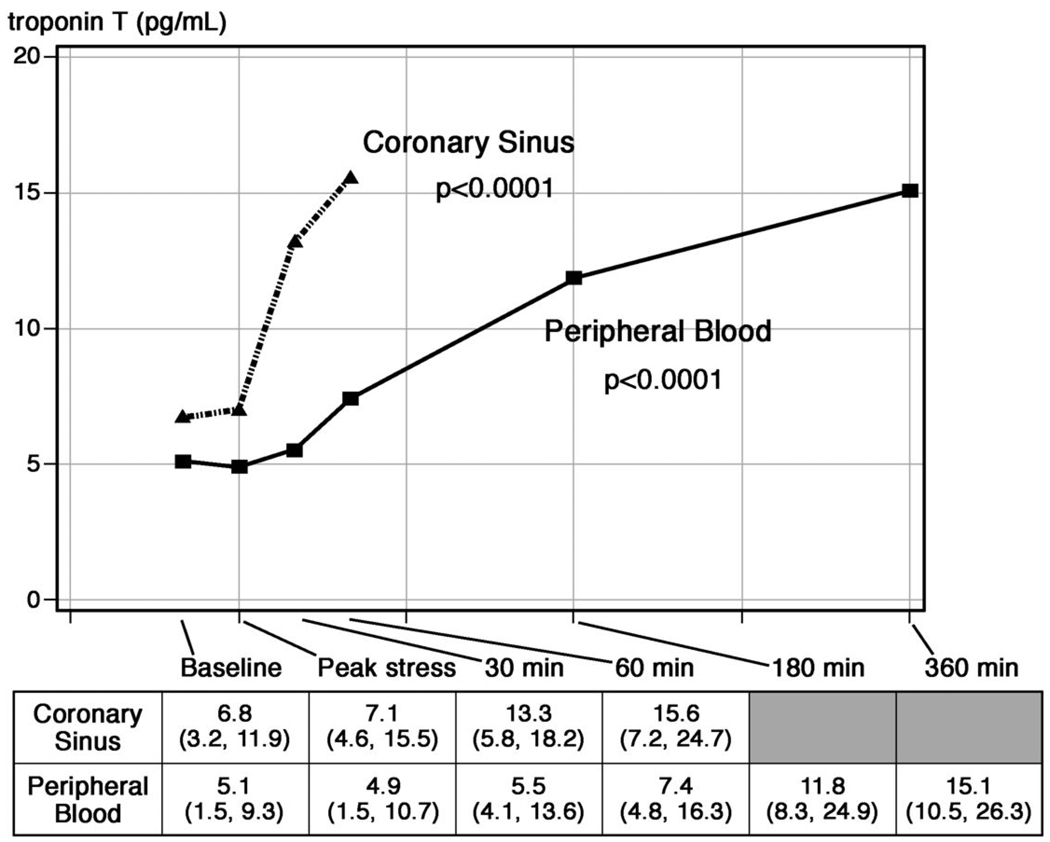
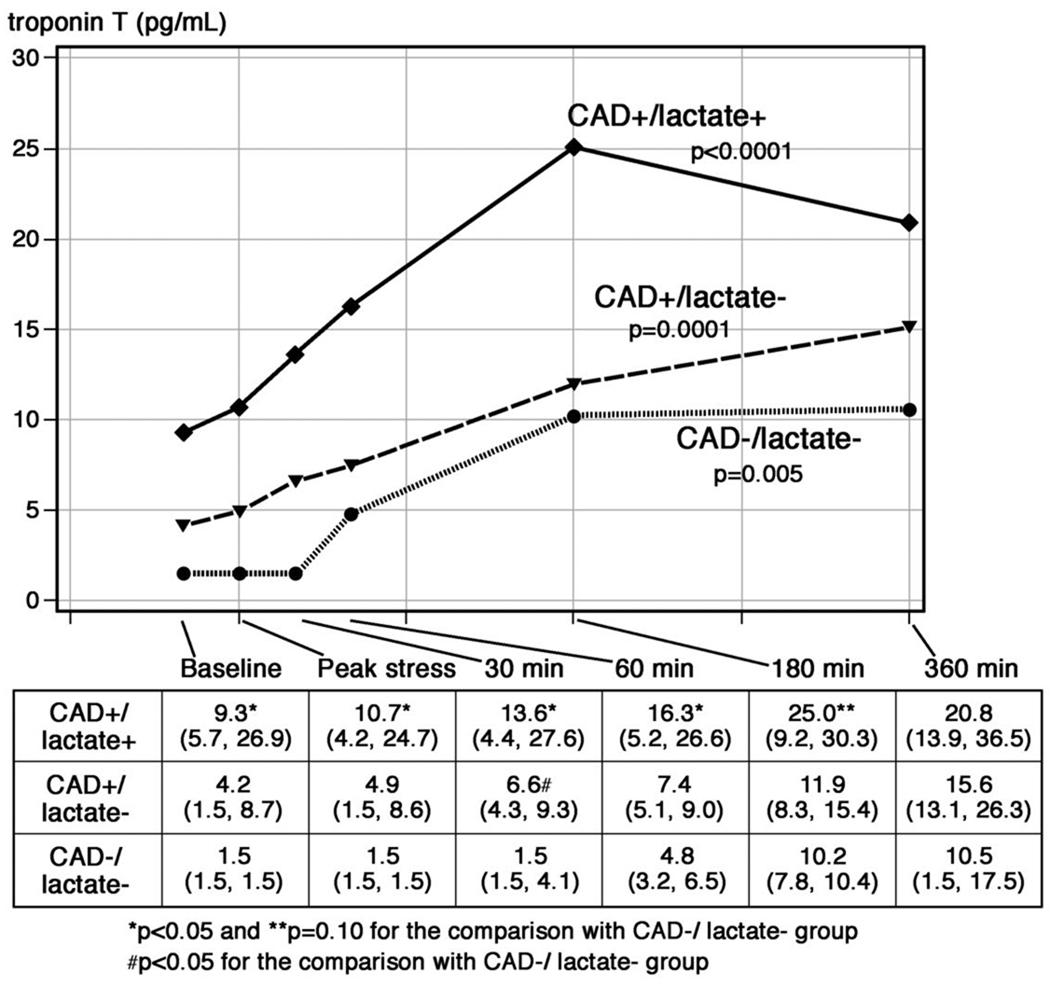
Results: cTnT concentrations in CS blood increased from a median of 6.8 pg/ml prior to pacing to 15.6 pg/ml 60 min after termination of rapid atrial pacing (p < 0.0001), changes that were mirrored at 180 min in peripheral blood (5.1 to 11.8 pg/ml, p < 0.0001). Although peripheral cTnT concentrations tended to be higher at 180 min following pacing for patients with CAD and lactate elution (n = 7) when compared with those without either marker (n = 5) (25.0 pg/ml vs. 10.2 pg/ml, p = 0.10), relative (1.7-fold vs. 5.2-fold) and absolute (6.8 pg/ml vs. 8.8 pg/ml, p = 0.50) changes were not different between groups.
Conclusions: Brief periods of ischemia, without frank infarction, cause low-level cTnT release, and small increases are common after periods of increased myocardial work, even among patients without objective evidence of myocardial ischemia or obstructive CAD. Additional research is needed before hs-cTnT assays are widely adopted in the management of subjects with chest pain syndromes.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Pathobiology of troponin elevations: do elevations occur with myocardial ischemia as well as necrosis?J Am Coll Cardiol. 2011 Jun 14;57(24):2406-8. doi: 10.1016/j.jacc.2011.01.029. J Am Coll Cardiol. 2011. PMID: 21658560 No abstract available.
References
-
- Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50:2173–2195. - PubMed
-
- Morrow DA, Cannon CP, Jesse RL, et al. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Circulation. 2007;115:e356–e375. - PubMed
-
- Eggers KM, Lagerqvist B, Venge P, Wallentin L, Lindahl B. Persistent cardiac troponin I elevation in stabilized patients after an episode of acute coronary syndrome predicts long-term mortality. Circulation. 2007;116:1907–1914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
