

Racial and ethnic differences in the association of body mass index and survival in maintenance hemodialysis patients
- PMID: 21658829
- PMCID: PMC3183288
- DOI: 10.1053/j.ajkd.2011.03.023
Racial and ethnic differences in the association of body mass index and survival in maintenance hemodialysis patients
Abstract
Background: In maintenance hemodialysis (HD) patients, overweight and obesity are associated with survival advantages. Given the greater survival of maintenance HD patients who are minorities, we hypothesized that increased body mass index (BMI) is associated more strongly with lower mortality in blacks and Hispanics relative to non-Hispanic whites.
Study design: Retrospective cohort study.
Setting & participants: We examined a 6-year (2001-2007) cohort of 109,605 maintenance HD patients including 39,090 blacks, 17,417 Hispanics, and 53,098 non-Hispanic white maintenance HD outpatients from DaVita dialysis clinics. Cox proportional hazards models examined the association between BMI and survival.
Predictors: Race and BMI.
Outcomes: All-cause mortality.
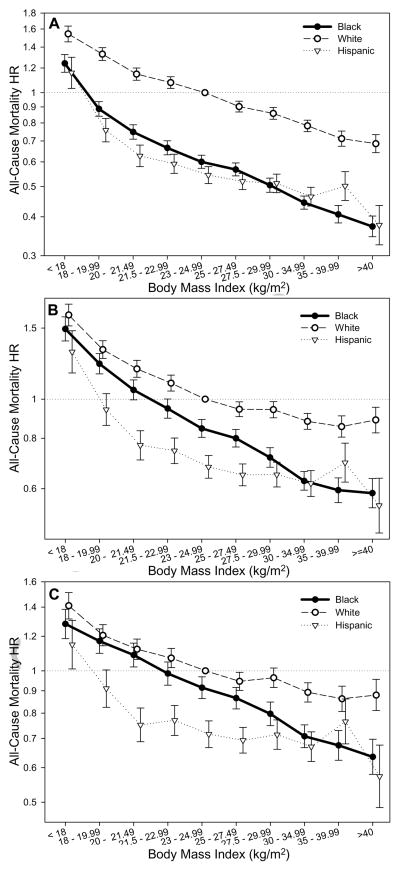
Results: Patients had a mean age of 62 ± 15 (standard deviation) years and included 45% women and 45% patients with diabetes. Across 10 a priori-selected BMI categories (<18-≥40 kg/m(2)), higher BMI was associated with greater survival in all 3 racial/ethnic groups. However, Hispanic and black patients experienced higher survival gains compared with non-Hispanic whites across higher BMI categories. Hispanics and blacks in the ≥40-kg/m(2) category had the largest adjusted decrease in death HR with increasing BMI (0.57 [95% CI, 0.49-0.68] and 0.63 [95% CI, 0.58-0.70], respectively) compared with non-Hispanic whites in the 23- to 25-kg/m(2) group (reference category). In linear models, although the inverse BMI-mortality association was observed for all subgroups, overall black maintenance HD patients showed the largest consistent decrease in death HR with increasing BMI.
Limitations: Race and ethnicity categories were based on self-identified data.
Conclusions: Whereas the survival advantage of high BMI is consistent across all racial/ethnic groups, black maintenance HD patients had the strongest and most consistent association of higher BMI with improved survival.
Copyright © 2011 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, Ishani A, et al. United States Renal Data System 2008 Annual Data Report. Am J Kidney Dis. 2009;53(1 Suppl):S1–374. - PubMed
-
- Wong JS, Port FK, Hulbert-Shearon TE, Carroll CE, Wolfe RA, Agodoa LY, et al. Survival advantage in Asian American end-stage renal disease patients. Kidney Int. 1999;55(6):2515–2523. - PubMed
-
- Tanna MM, Vonesh EF, Korbet SM. Patient survival among incident peritoneal dialysis and hemodialysis patients in an urban setting. Am J Kidney Dis. 2000;36(6):1175–1182. - PubMed
