

The marginal value of pre-visit paper reminders when added to a multifaceted electronic health record based quality improvement system
- PMID: 21659446
- PMCID: PMC3197995
- DOI: 10.1136/amiajnl-2011-000169
The marginal value of pre-visit paper reminders when added to a multifaceted electronic health record based quality improvement system
Abstract
Objective: We have reported that implementation of an electronic health record (EHR) based quality improvement system that included point-of-care electronic reminders accelerated improvement in performance for multiple measures of chronic disease care and preventive care during a 1-year period. This study examined whether providing pre-visit paper quality reminders could further improve performance, especially for physicians whose performance had not improved much during the first year.
Design: Time-series analysis at a large internal medicine practice using a commercial EHR. All patients eligible for each measure were included (range approximately 100-7500).
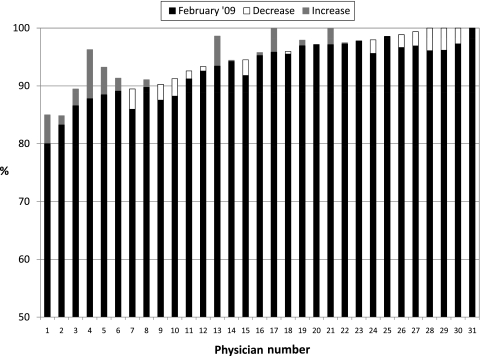
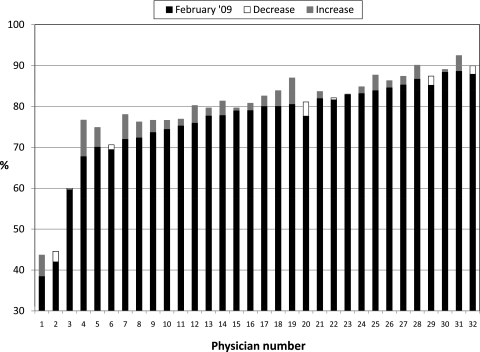
Measurements: The proportion of eligible patients in the practice who satisfied each of 15 quality measures after removing those with exceptions from the denominator. To analyze changes in performance for individual physicians, two composite measures were used: prescribing seven essential medications and completion of five preventive services.
Results: During the year after implementing pre-encounter reminders, performance continued to improve for eight measures, remained stable for four, and declined for three. Physicians with the worst performance at the start of the pre-encounter reminders showed little absolute improvement over the next year, and most remained below the median performance for physicians in the practice.
Conclusions: Paper pre-encounter reminders did not appear to improve performance beyond electronic point-of-care reminders in the EHR alone. Lagging performance is likely not due to providers' EHR workflow alone, and trying to step backwards and use paper reminders in addition to point-of-care reminders in the EHR may not be an effective strategy for engaging slow adopters.
Conflict of interest statement
Figures
References
-
- Kerr EA, Smith DM, Hogan MM, et al. Comparing clinical automated, medical record, and hybrid data sources for diabetes quality measures. Jt Comm J Qual Improv 2002;28:555–65 - PubMed
-
- Chaudhry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med 2006;144:742–52 - PubMed
-
- Persell SD, Kaiser D, Dolan NC, et al. Changes in performance after implementation of a multifaceted electronic-health-record-based quality improvement system. Med Care 2011;49:117–25 - PubMed
