

Risk of brain tumours in relation to estimated RF dose from mobile phones: results from five Interphone countries
- PMID: 21659469
- PMCID: PMC3158328
- DOI: 10.1136/oemed-2011-100155
Risk of brain tumours in relation to estimated RF dose from mobile phones: results from five Interphone countries
Abstract
Objectives: The objective of this study was to examine the associations of brain tumours with radio frequency (RF) fields from mobile phones.
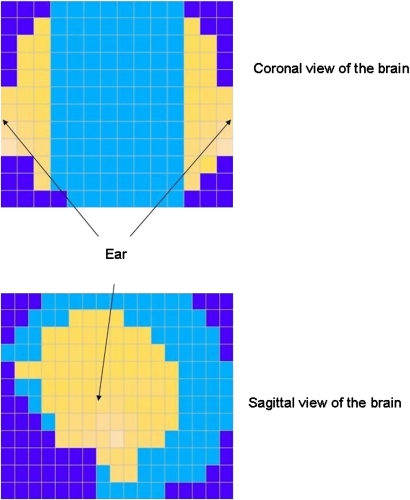
Methods: Patients with brain tumour from the Australian, Canadian, French, Israeli and New Zealand components of the Interphone Study, whose tumours were localised by neuroradiologists, were analysed. Controls were matched on age, sex and region and allocated the 'tumour location' of their matched case. Analyses included 553 glioma and 676 meningioma cases and 1762 and 1911 controls, respectively. RF dose was estimated as total cumulative specific energy (TCSE; J/kg) absorbed at the tumour's estimated centre taking into account multiple RF exposure determinants.
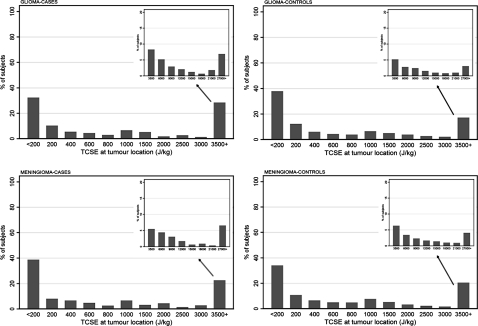
Results: ORs with ever having been a regular mobile phone user were 0.93 (95% CI 0.73 to 1.18) for glioma and 0.80 (95% CI 0.66 to 0.96) for meningioma. ORs for glioma were below 1 in the first four quintiles of TCSE but above 1 in the highest quintile, 1.35 (95% CI 0.96 to 1.90). The OR increased with increasing TCSE 7+ years before diagnosis (p-trend 0.01; OR 1.91, 95% CI 1.05 to 3.47 in the highest quintile). A complementary analysis in which 44 glioma and 135 meningioma cases in the most exposed area of the brain were compared with gliomas and meningiomas located elsewhere in the brain showed increased ORs for tumours in the most exposed part of the brain in those with 10+ years of mobile phone use (OR 2.80, 95% CI 1.13 to 6.94 for glioma). Patterns for meningioma were similar, but ORs were lower, many below 1.0.
Conclusions: There were suggestions of an increased risk of glioma in long-term mobile phone users with high RF exposure and of similar, but apparently much smaller, increases in meningioma risk. The uncertainty of these results requires that they be replicated before a causal interpretation can be made.
Conflict of interest statement
Figures
Comment in
-
Interphone, IARC and radiofrequency fields: where to next?Occup Environ Med. 2011 Sep;68(9):629-30. doi: 10.1136/oemed-2011-100358. Occup Environ Med. 2011. PMID: 21835976 No abstract available.
References
-
- Cardis E, Richardson L, Deltour I, et al. The INTERPHONE study: design, epidemiological methods, and description of the study population. Eur J Epidemiol 2007;22:647–64 - PubMed
-
- Dreyer NA, Loughlin JE, Rothman KJ. Cause-specific mortality in cellular telephone users. JAMA 1999;282:1814–16 - PubMed
-
- Johansen C, Boice J, Jr, McLaughlin J, et al. Cellular telephones and cancer–a nationwide cohort study in Denmark. J Natl Cancer Inst 2001;93:203–7 - PubMed
-
- Schüz J, Jacobsen R, Olsen JH, et al. Cellular telephone use and cancer risk: update of a nationwide Danish cohort. J Natl Cancer Inst 2006;98:1707–13 - PubMed
-
- Auvinen A, Hietanen M, Luukkonen R, et al. Brain tumors and salivary gland cancers among cellular telephone users. Epidemiology 2002;13:356–9 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical