

Long-term outcome and lineage-specific chimerism in 194 patients with Wiskott-Aldrich syndrome treated by hematopoietic cell transplantation in the period 1980-2009: an international collaborative study
- PMID: 21659547
- PMCID: PMC3156052
- DOI: 10.1182/blood-2010-11-319376
Long-term outcome and lineage-specific chimerism in 194 patients with Wiskott-Aldrich syndrome treated by hematopoietic cell transplantation in the period 1980-2009: an international collaborative study
Abstract
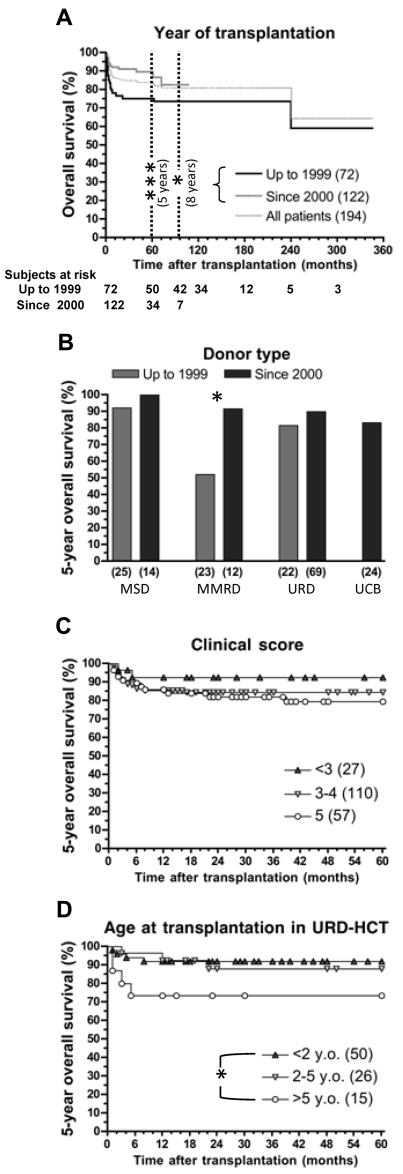
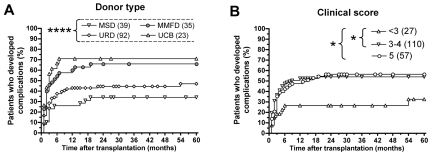
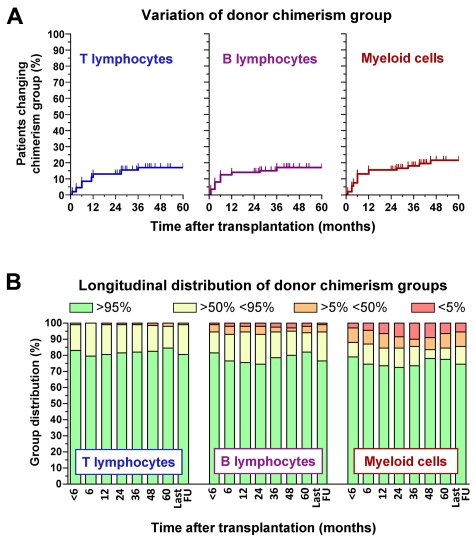
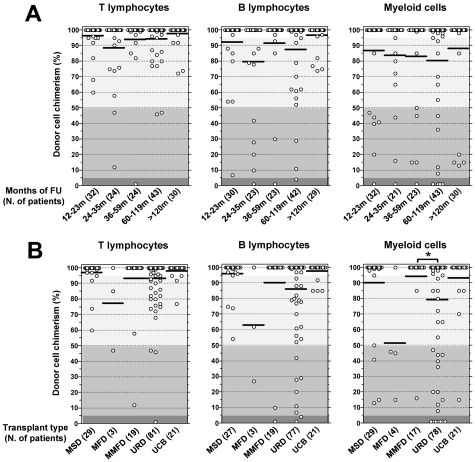
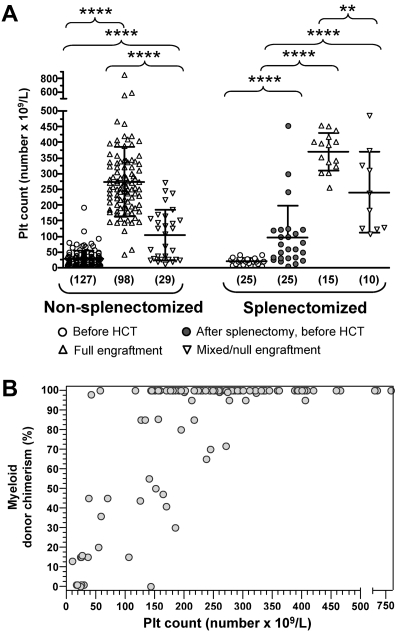
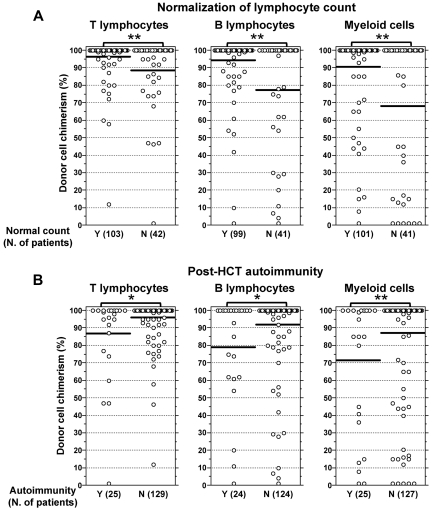
In this retrospective collaborative study, we have analyzed long-term outcome and donor cell engraftment in 194 patients with Wiskott-Aldrich syndrome (WAS) who have been treated by hematopoietic cell transplantation (HCT) in the period 1980- 2009. Overall survival was 84.0% and was even higher (89.1% 5-year survival) for those who received HCT since the year 2000, reflecting recent improvement of outcome after transplantation from mismatched family donors and for patients who received HCT from an unrelated donor at older than 5 years. Patients who went to transplantation in better clinical conditions had a lower rate of post-HCT complications. Retrospective analysis of lineage-specific donor cell engraftment showed that stable full donor chimerism was attained by 72.3% of the patients who survived for at least 1 year after HCT. Mixed chimerism was associated with an increased risk of incomplete reconstitution of lymphocyte count and post-HCT autoimmunity, and myeloid donor cell chimerism < 50% was associated with persistent thrombocytopenia. These observations indicate continuous improvement of outcome after HCT for WAS and may have important implications for the development of novel protocols aiming to obtain full correction of the disease and reduce post-HCT complications.
Figures
References
-
- Ochs HD, Filipovich AH, Veys P, Cowan MJ, Kapoor N. Wiskott-Aldrich syndrome: diagnosis, clinical and laboratory manifestations, and treatment. Biol Blood Marrow Transplant. 2009;15(1 suppl):84–90. - PubMed
-
- Ochs HD, Thrasher AJ. The Wiskott-Aldrich syndrome. J Allergy Clin Immunol. 2006;117(4):725–738. quiz 739. - PubMed
-
- Bosticardo M, Marangoni F, Aiuti A, Villa A, Grazia Roncarolo M. Recent advances in understanding the pathophysiology of Wiskott-Aldrich syndrome. Blood. 2009;113(25):6288–6295. - PubMed
-
- Derry JM, Ochs HD, Francke U. Isolation of a novel gene mutated in Wiskott-Aldrich syndrome. Cell. 1994;78(4):635–644. Erratum in: Cell. 1994;79(5):922. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
