

Prehospital notification by emergency medical services reduces delays in stroke evaluation: findings from the North Carolina stroke care collaborative
- PMID: 21659638
- PMCID: PMC3970287
- DOI: 10.1161/STROKEAHA.110.605857
Prehospital notification by emergency medical services reduces delays in stroke evaluation: findings from the North Carolina stroke care collaborative
Abstract
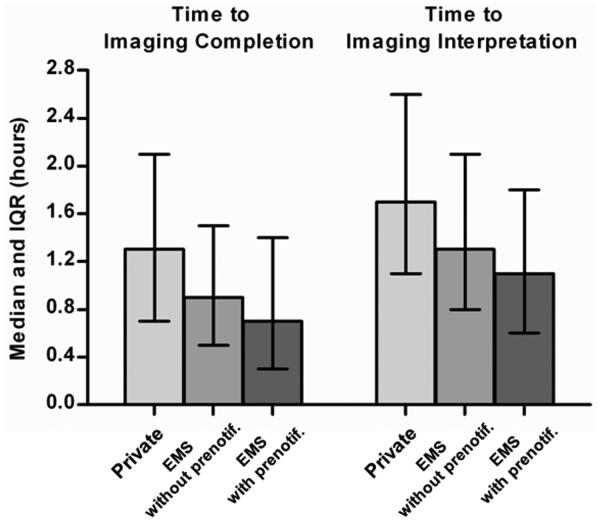
Background and purpose: Individuals with stroke-like symptoms are recommended to receive rapid diagnostic evaluation. Emergency medical services (EMS) transport, compared with private modes, and hospital notification before arrival may reduce delays in evaluation. This study estimated associations between hospital arrival modes (EMS or private and with or without EMS prenotification) and times for completion and interpretation of initial brain imaging in patients with presumed stroke.
Methods: Among patients with suspected stroke identified and enrolled by the North Carolina Stroke Care Collaborative registry in 2008 to 2009, we analyzed data on arrival modes, meeting recommended targets for brain imaging completion and interpretation times (<25 minutes and <45 minutes since hospital arrival, respectively) and patient- and hospital-level characteristics. We used modified Poisson regression to estimate adjusted risk ratios and 95% CIs.
Results: Of 13 894 eligible patients, 21% had their brain imaging completed and 23% had their brain imaging interpreted by a physician within target times. Arrival by EMS (versus private transport) was associated with both brain imaging completed within 25 minutes of arrival (EMS with prenotification: risk ratio, 3.0; 95% CI, 2.1 to 4.1; EMS without prenotification: risk ratio, 1.9; 95% CI, 1.6 to 2.3) and brain imaging interpreted within 45 minutes (EMS with prenotification: risk ratio, 2.7; 95% CI, 2.3 to 3.3; EMS without prenotification: risk ratio, 1.7; 95% CI, 1.4 to 2.1).
Conclusions: Patients with presumed stroke arriving to the hospital by EMS were more likely to receive brain imaging and have it interpreted by a physician in a timely manner than those arriving by private transport. Moreover, EMS arrivals with hospital prenotification experienced the most rapid evaluation.
Figures
References
-
- Adams HP, Jr., del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655–1711. - PubMed
-
- Marler JR, Tilley BC, Lu M, Brott TG, Lyden PC, Grotta JC, et al. Early stroke treatment associated with better outcome The NINDS rt-PA Stroke Study. Neurology. 2000;55:1649–1655. - PubMed
-
- Alberts MJ, Latchaw RE, Selman WR, Shephard T, Hadley MN, Brass LM, et al. Recommendations for Comprehensive Stroke Centers A Consensus Statement From the Brain Attack Coalition. Stroke. 2005;36:1597–1616. - PubMed
-
- Reeves MJ, Broderick JP, Frankel M, LaBresh KA, Schwamm L, Moomaw CJ, et al. The Paul Coverdell National Acute Stroke Registry Initial Results from Four Prototypes. American Journal of Preventive Medicine. 2006;31:202–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
