

doi: 10.1172/JCI45449.
Cytomegalovirus: pathogen, paradigm, and puzzle
Affiliations
- PMID: 21659716
- PMCID: PMC3083799
- DOI: 10.1172/JCI45449
Item in Clipboard
Cytomegalovirus: pathogen, paradigm, and puzzle
J Clin Invest.
2011 May.
Abstract
Human cytomegalovirus (CMV), one of the eight herpesviruses that commonly infect humans, is best known for its propensity to cause disease in immunocompromised patients, especially transplant recipients, patients with advanced AIDS, and congenitally infected newborns. Advances in molecular virology coupled with improvements in diagnostic methods and treatment options have vastly improved our understanding of and ability to manage CMV, but many uncertainties remain, including the mechanisms of persistence and pathogenesis and its hypothesized roles in a variety of human illnesses. Here we review recent advances that are reshaping our view and approach to this fascinating virus.
Figures
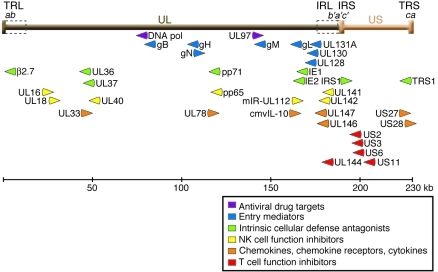
The genome of CMV clinical isolates, such as the Merlin strain depicted here (GenBank accession no. NC_006273; ref. 118), consists of long (brown) and short (orange) DNA segments, each of which has unique regions (UL and US) flanked by inverted repeats (TRL/IRL and IRS/TRS). These repeats contain segment-specific sequences (b, b′, c, and c′) as well as a variable number of shared a sequence repeats in direct orientation at the genomic ends and in an inverted orientation at the junction of the two segments. Laboratory-adapted strains often have deletions of multiple genes at the right end of the UL segment and their replacement with genes duplicated from the left end, resulting in longer TRL and IRL regions (dashed boxes) compared with clinical strains (21, 118). The gene names in this region are not always sequential because of historical precedence in nomenclature assignments and because of rearrangements among strains. The relative position and orientation of transcripts corresponding to several genes are shown, along with grouping by their putative functional classifications (, , –45, 47). This diagram is a simplification, since some and possibly many of the genes shown here have more than one function and other genes that are not shown likely contribute to the indicated processes.
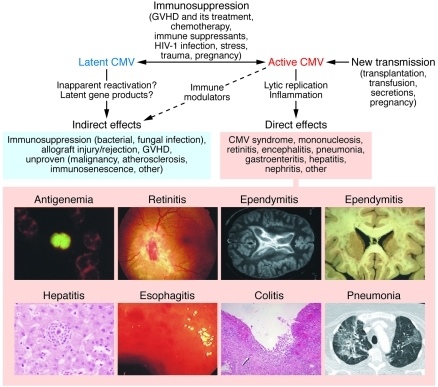
Many humans harbor clinically quiescent or latent CMV. Even when asymptomatic, the virus may cause indirect effects, possibly by altering immune system function after subclinical reactivation episodes or by expression of viral genes (e.g., LAcmvIl-10) during latency. Immune system dysfunction resulting from a variety of iatrogenic or natural causes or from a new transmission event can lead to active CMV replication. Depending on the clinical setting, active replication may contribute to indirect effects, but also leads to direct tissue damage, resulting in an inflammatory response and dysfunction of various organ systems. In addition to CMV antigenemia, a common indicator of active infection, examples of end CMV organ disease commonly occurring in AIDS patients and in transplant recipients are shown. Image credits: antigenemia, pp65+ cell in a leukocyte cytospin preparation (M. Boeckh); retinitis, ophthalmoscopic view of retinal hemorrhage and inflammation (E. Chuang); ependymitis, periventricular inflammation detected by MRI (left; reproduced from ref. with permission from McGraw Hill) and postmortem brain specimen (right; C. Marra); hepatitis, microabscesses associated with CMV hepatitis (A. Limaye); esophagitis, endoscopic view of shallow esophageal ulcers (G. McDonald); colitis, deep ulcer in a colonic biopsy (G. McDonald); pneumonia, chest CT scan of CMV pneumonia (M. Boeckh).
References
-
- Rippert H. Uber protozoenartige Zellen in der Niere eines syphilitischen Neugoborenen und in der Parotis von Kindern. Zentralbl Allg Pathol. 1904;15:945–948.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
