

Incidence and predictors of microbiology results returning postdischarge and requiring follow-up
- PMID: 21661103
- PMCID: PMC3779697
- DOI: 10.1002/jhm.895
Incidence and predictors of microbiology results returning postdischarge and requiring follow-up
Abstract
Background: Failure to follow up microbiology results pending at discharge can delay appropriate treatment, increasing the risk of patient harm and litigation. Limited data describe the frequency of postdischarge microbiology results requiring a treatment change.
Objective: To determine the incidence and predictors of postdischarge microbiology results requiring follow-up.
Design: Cross-sectional.
Setting: Large academic hospital during 2007.
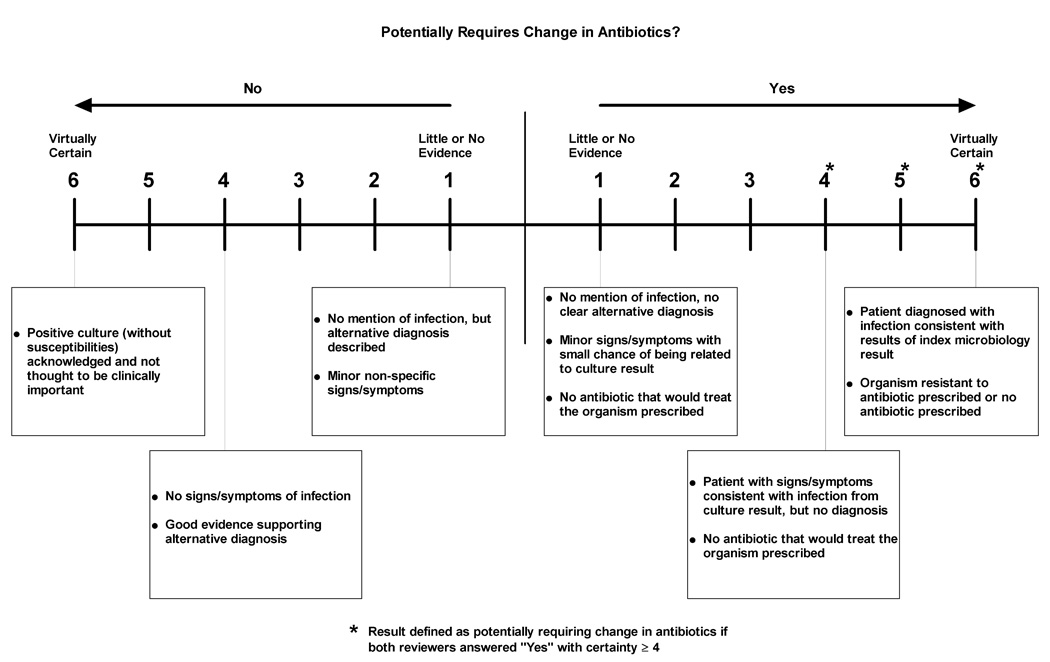
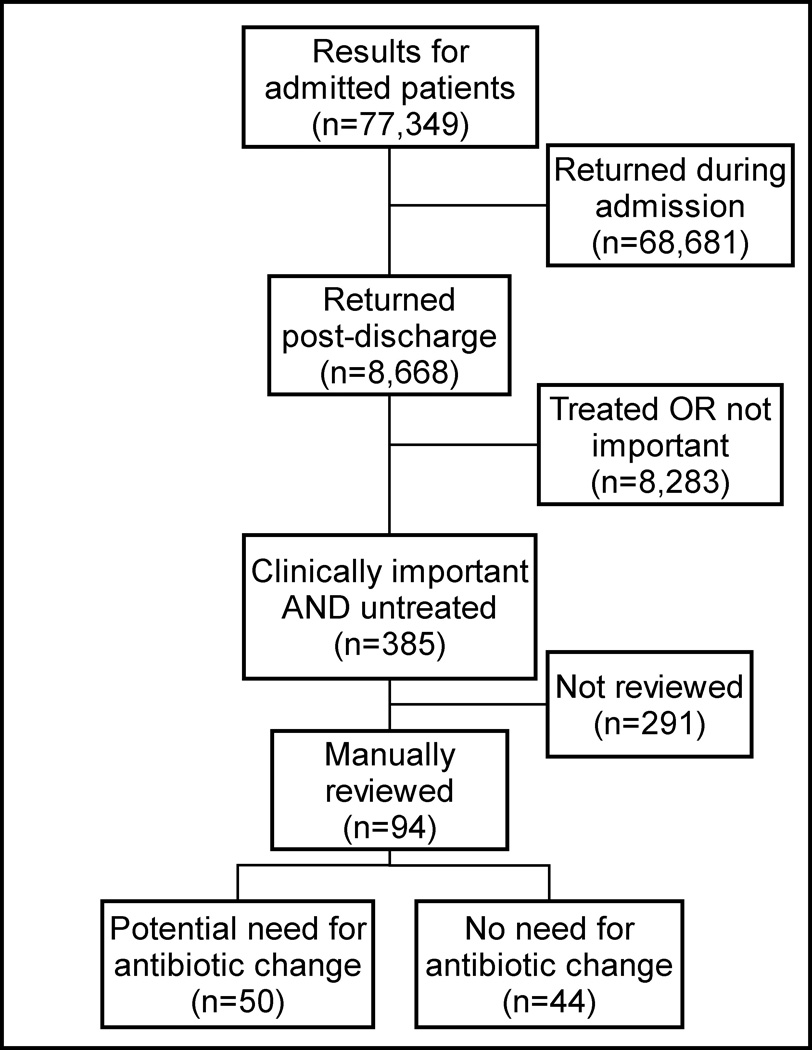
Measurements: We evaluated blood, urine, sputum, and cerebrospinal fluid (CSF) cultures ordered for hospitalized patients. We identified cultures that returned postdischarge and determined which were clinically important and not treated by an antibiotic to which they were susceptible. We reviewed a random subset to assess the potential need for antibiotic change. Using logistic regression, we identified significant predictors of results requiring follow-up.
Results: Of 77,349 inpatient culture results, 8668 (11%) returned postdischarge. Of these, 385 (4%) were clinically important and untreated at discharge. Among 94 manually reviewed cases, 53% potentially required a change in therapy. Urine cultures were more likely to potentially require therapy change than non-urine cultures (OR 2.8, 95% CI 1.1-7.2; P = 0.03). Also, 76% of 25 results from surgical services potentially required a therapy change, compared with 59% of 29 results from general medicine, 38% of 16 results from oncology, and 33% of 24 results from medical subspecialties. Overall, 2.4% of postdischarge cultures potentially necessitated an antibiotic change.
Conclusions: Many microbiology results return postdischarge and some necessitate a change in treatment. These results arise from many specialties, suggesting the need for a hospital-wide system to ensure effective communication of these results.
Copyright © 2010 Society of Hospital Medicine.
Conflict of interest statement
Dr. El-Kareh had full access to all the data in the study and takes responsibility for the integrity and the accuracy of the data analysis. The authors have no conflicts of interest to disclose.
Figures
References
-
- Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005 Jul 19;143(2):121–128. - PubMed
-
- Bates DW, Leape LL. Doing better with critical test results. Jt Comm J Qual Patient Saf. 2005 Feb;31(2):66–67. 61. - PubMed
-
- Gandhi TK. Fumbled handoffs: one dropped ball after another. Ann Intern Med. 2005 Mar 1;142(5):352–358. - PubMed
-
- Hanna D, Griswold P, Leape LL, Bates DW. Communicating critical test results: safe practice recommendations. Jt Comm J Qual Patient Saf. 2005 Feb;31(2):68–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
