

The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial
- PMID: 21663949
- PMCID: PMC3145073
- DOI: 10.1016/S0140-6736(11)60739-3
The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial
Abstract
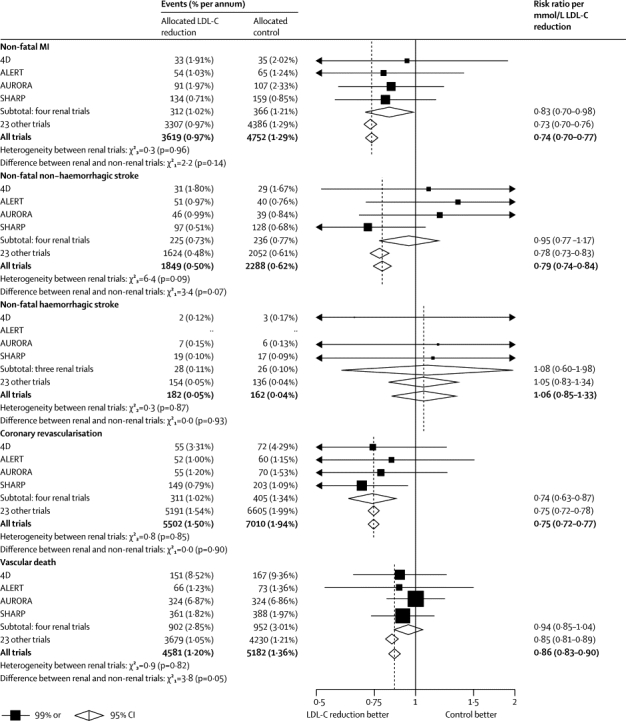
Background: Lowering LDL cholesterol with statin regimens reduces the risk of myocardial infarction, ischaemic stroke, and the need for coronary revascularisation in people without kidney disease, but its effects in people with moderate-to-severe kidney disease are uncertain. The SHARP trial aimed to assess the efficacy and safety of the combination of simvastatin plus ezetimibe in such patients.
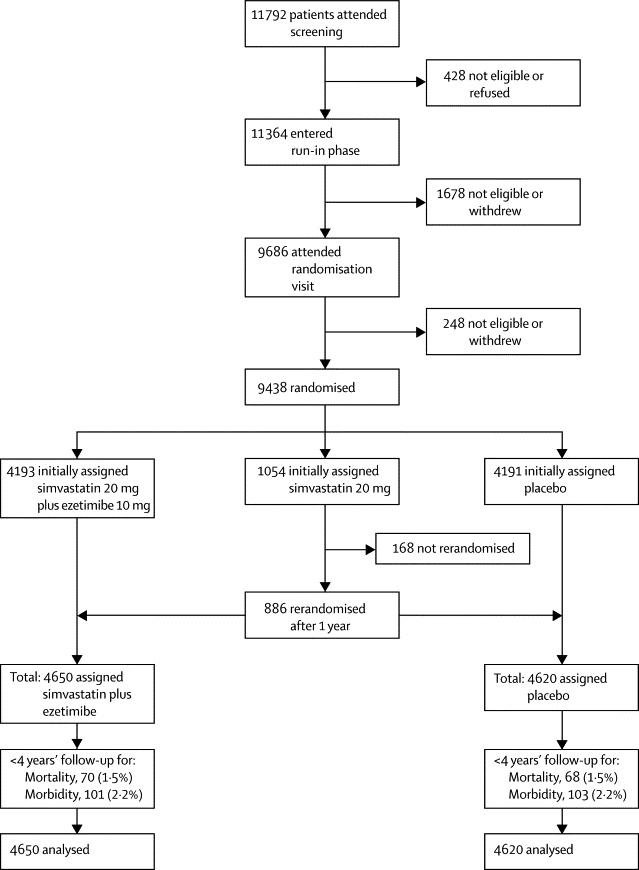
Methods: This randomised double-blind trial included 9270 patients with chronic kidney disease (3023 on dialysis and 6247 not) with no known history of myocardial infarction or coronary revascularisation. Patients were randomly assigned to simvastatin 20 mg plus ezetimibe 10 mg daily versus matching placebo. The key prespecified outcome was first major atherosclerotic event (non-fatal myocardial infarction or coronary death, non-haemorrhagic stroke, or any arterial revascularisation procedure). All analyses were by intention to treat. This trial is registered at ClinicalTrials.gov, NCT00125593, and ISRCTN54137607.
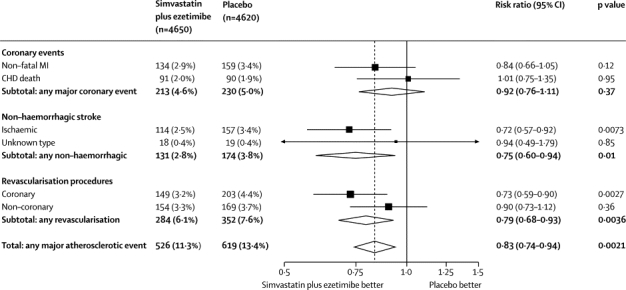
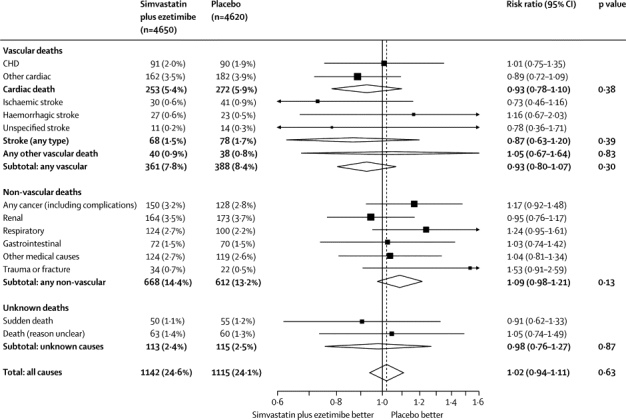
Findings: 4650 patients were assigned to receive simvastatin plus ezetimibe and 4620 to placebo. Allocation to simvastatin plus ezetimibe yielded an average LDL cholesterol difference of 0·85 mmol/L (SE 0·02; with about two-thirds compliance) during a median follow-up of 4·9 years and produced a 17% proportional reduction in major atherosclerotic events (526 [11·3%] simvastatin plus ezetimibe vs 619 [13·4%] placebo; rate ratio [RR] 0·83, 95% CI 0·74-0·94; log-rank p=0·0021). Non-significantly fewer patients allocated to simvastatin plus ezetimibe had a non-fatal myocardial infarction or died from coronary heart disease (213 [4·6%] vs 230 [5·0%]; RR 0·92, 95% CI 0·76-1·11; p=0·37) and there were significant reductions in non-haemorrhagic stroke (131 [2·8%] vs 174 [3·8%]; RR 0·75, 95% CI 0·60-0·94; p=0·01) and arterial revascularisation procedures (284 [6·1%] vs 352 [7·6%]; RR 0·79, 95% CI 0·68-0·93; p=0·0036). After weighting for subgroup-specific reductions in LDL cholesterol, there was no good evidence that the proportional effects on major atherosclerotic events differed from the summary rate ratio in any subgroup examined, and, in particular, they were similar in patients on dialysis and those who were not. The excess risk of myopathy was only two per 10,000 patients per year of treatment with this combination (9 [0·2%] vs 5 [0·1%]). There was no evidence of excess risks of hepatitis (21 [0·5%] vs 18 [0·4%]), gallstones (106 [2·3%] vs 106 [2·3%]), or cancer (438 [9·4%] vs 439 [9·5%], p=0·89) and there was no significant excess of death from any non-vascular cause (668 [14·4%] vs 612 [13·2%], p=0·13).
Interpretation: Reduction of LDL cholesterol with simvastatin 20 mg plus ezetimibe 10 mg daily safely reduced the incidence of major atherosclerotic events in a wide range of patients with advanced chronic kidney disease.
Funding: Merck/Schering-Plough Pharmaceuticals; Australian National Health and Medical Research Council; British Heart Foundation; UK Medical Research Council.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures


Comment in
-
SHARP: a stab in the right direction in chronic kidney disease.Lancet. 2011 Jun 25;377(9784):2153-4. doi: 10.1016/S0140-6736(11)60822-2. Epub 2011 Jun 12. Lancet. 2011. PMID: 21663950 No abstract available.
-
Vascular disease: lowering LDL cholesterol reduces atherosclerotic risk in patients with chronic kidney disease.Nat Rev Cardiol. 2011 Jun 28;8(8):424. doi: 10.1038/nrcardio.2011.100. Nat Rev Cardiol. 2011. PMID: 21709703 No abstract available.
-
Benefits of lowering cholesterol in chronic kidney disease.Lancet. 2011 Oct 15;378(9800):1375; author reply 1377-8. doi: 10.1016/S0140-6736(11)61604-8. Lancet. 2011. PMID: 22000127 No abstract available.
-
Benefits of lowering cholesterol in chronic kidney disease.Lancet. 2011 Oct 15;378(9800):1376; author reply 1377-8. doi: 10.1016/S0140-6736(11)61606-1. Lancet. 2011. PMID: 22000129 No abstract available.
-
Benefits of lowering cholesterol in chronic kidney disease.Lancet. 2011 Oct 15;378(9800):1376-7; author reply 1377-8. doi: 10.1016/S0140-6736(11)61607-3. Lancet. 2011. PMID: 22000130 No abstract available.
-
Benefits of lowering cholesterol in chronic kidney disease.Lancet. 2011 Oct 15;378(9800):1376; author reply 1377-8. doi: 10.1016/S0140-6736(11)61605-X. Lancet. 2011. PMID: 22000131 No abstract available.
-
Lipid-lowering therapy in individuals with CKD: lessons learned from SHARP.Am J Kidney Dis. 2012 Feb;59(2):170-3. doi: 10.1053/j.ajkd.2011.09.008. Epub 2011 Oct 26. Am J Kidney Dis. 2012. PMID: 22033284 No abstract available.
-
ACP Journal Club. Simvastatin plus ezetimibe reduced major atherosclerotic events in patients with chronic kidney disease.Ann Intern Med. 2011 Nov 15;155(10):JC5-02. doi: 10.7326/0003-4819-155-10-201111150-02002. Ann Intern Med. 2011. PMID: 22084349 No abstract available.
-
Lipid lowering in patients with chronic kidney disease: a SHARP turn in the wrong direction?Eur J Cardiovasc Prev Rehabil. 2011 Dec;18(6):858-61. doi: 10.1177/1741826711423116. Eur J Cardiovasc Prev Rehabil. 2011. PMID: 22087046
-
A sharp study, but with blunted conclusions.Semin Dial. 2011 Nov-Dec;24(6):684-5. doi: 10.1111/j.1525-139X.2011.01002.x. Semin Dial. 2011. PMID: 22151530 No abstract available.
References
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(suppl 3):S112–S119. - PubMed
-
- National Kidney Foundation K/DOQI clinical practice guidelines for managing dyslipidemias in chronic kidney disease. Am J Kidney Dis. 2003;41(suppl 3):S1–91. - PubMed
-
- Cholesterol Treatment Trialists' (CTT) Collaborators Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
