

Preoperative pulmonary rehabilitation before lung cancer resection: results from two randomized studies
- PMID: 21663994
- PMCID: PMC3191236
- DOI: 10.1016/j.lungcan.2011.05.011
Preoperative pulmonary rehabilitation before lung cancer resection: results from two randomized studies
Abstract
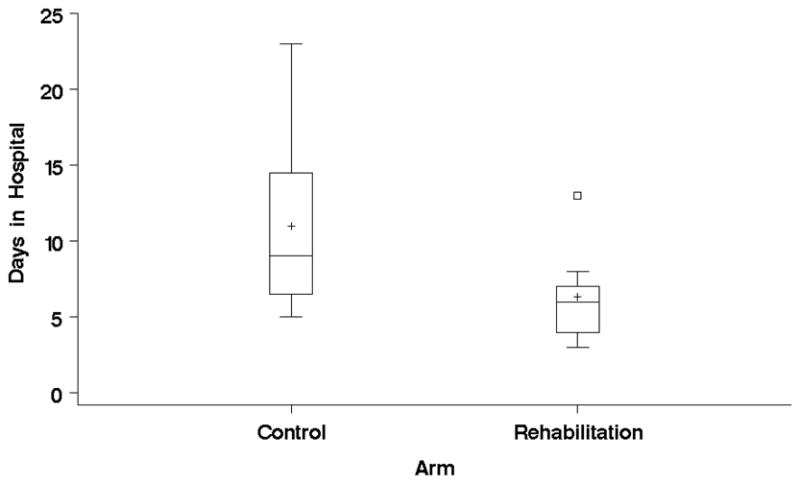
Complete surgical resection is the most effective curative treatment for lung cancer. However, many patients with lung cancer also have severe COPD which increases their risk of postoperative complications and their likelihood of being considered "inoperable." Preoperative pulmonary rehabilitation (PR) has been proposed as an intervention to decrease surgical morbidity but there is no established protocol and no randomized study has been published to date. We tested two preoperative PR interventions in patients undergoing lung cancer resection and with moderate-severe COPD in a randomized single blinded design. Outcomes were length of hospital stay and postoperative complications. The first study tested 4 weeks of guideline-based PR vs. usual care: that study proved to be very difficult to recruit as patients and providers were reluctant to delay surgery. Nine patients were randomized and no differences were found between arms. The second study tested ten preoperative PR sessions using a customized protocol with nonstandard components (exercise prescription based on self efficacy, inspiratory muscle training, and the practice of slow breathing) (n=10) vs. usual care (n=9). The PR arm had shorter length of hospital stay by 3 days (p=0.058), fewer prolonged chest tubes (11% vs. 63%, p=0.03) and fewer days needing a chest tube (8.8 vs. 4.3 days p=0.04) compared to the controlled arm. A ten-session preoperative PR intervention may improve post operative lung reexpansion evidenced by shorter chest tube times and decrease the length of hospital stay, a crude estimator of post operative morbidity and costs. Our results suggest the potential for short term preoperative pulmonary rehabilitation interventions in patients with moderate-severe COPD undergoing curative lung resection. 4 weeks of conventional preoperative PR seems non feasible.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
“Conflict of interest statement”
None declared by any of the authors
Figures
References
-
- Licker MJ, Widikker I, Robert J, et al. Operative mortality and respiratory complications after lung resection for cancer: impact of chronic obstructive pulmonary disease and time trends. Ann Thorac Surg. 2006;81:1830–1837. - PubMed
-
- Bolliger CT, Jordan P, Soler M, et al. Exercise capacity as a predictor of postoperative complications in lung resection candidates. Am J Respir Crit Care Med. 1995;151:1472–1480. - PubMed
-
- Win T, Jackson A, Groves AM, et al. Relationship of shuttle walk test and lung cancer surgical outcome. Eur J Cardiothorac Surg. 2004;26:1216–1219. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
