

Genetic counseling for isolated GnRH deficiency
- PMID: 21664415
- PMCID: PMC3185214
- DOI: 10.1016/j.mce.2011.05.041
Genetic counseling for isolated GnRH deficiency
Abstract
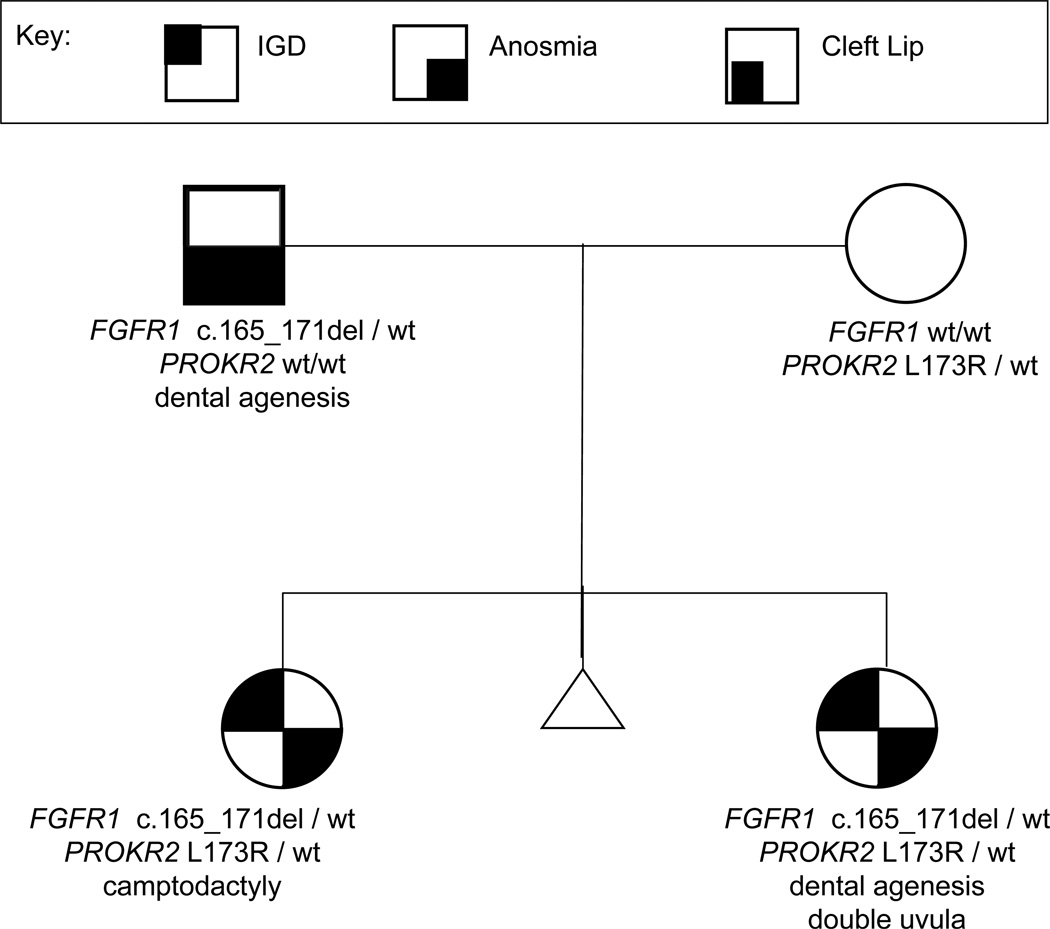
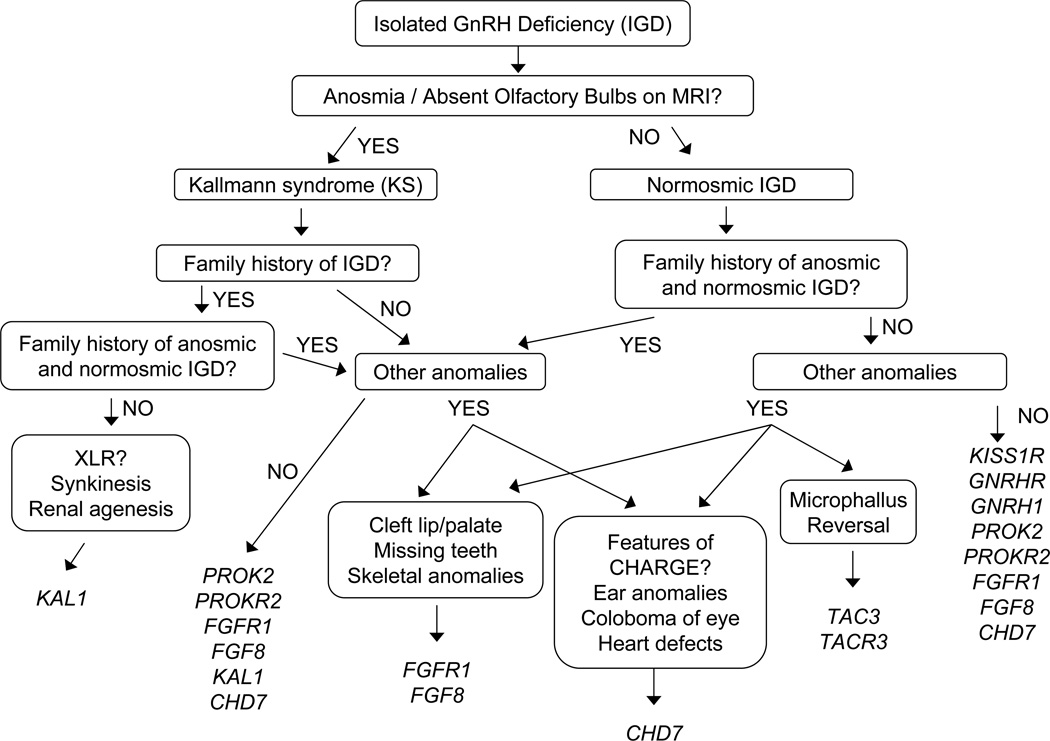
As our understanding of the complexities of the various etiologies and complex genetic architecture of GnRH deficiency grows, so too does the need to apply newly-developed genetic tools in a way that: (a) is meaningful to individuals and their families; (b) integrates all of the phenotypic features of this syndrome into a rationale; and (c) provides up-to-date diagnostic technologies in a cost-effective algorithm of genetic testing. Genetic counseling aims to accomplish these goals through ascertainment of detailed family histories, targeted comprehensive phenotypic evaluations, informed selection of genetic testing, interpretation of genetic test results, and the provision of highly specific risk assessments and psychological support to individuals diagnosed with this reproductive condition. This chapter offers a guide to incorporating this rapidly evolving state of knowledge of the pedigree and phenotypes into the process of selecting and prioritizing genetic testing. In addition, the provision of risk assessment that accounts for nuanced genetic concepts such as variable expressivity, incomplete penetrance, and oligogenicity, all of which are emerging features of the genetics of this clinical syndrome, is considered. Beyond translating genetic information, genetic counseling should address the psychological impact of embarrassment, shame, anxiety, and guilt that are often seen among individuals with reproductive disorders.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Abreu AP, Trarbach EB, de Castro M, Frade Costa EM, Versiani B, Matias Baptista MT, Garmes HM, Mendonca BB, Latronico AC. Loss-of-function mutations in the genes encoding prokineticin-2 or prokineticin receptor-2 cause autosomal recessive Kallmann syndrome. J. Clin. Endocrinol. Metab. 2008;93:4113–4118. - PubMed
-
- Baum A, Friedman AL, Zakowski SG. Stress and Genetic Testing for Disease Risk. Health Psychology. 1997;16(1):8–19. - PubMed
-
- Bédécarrats GY, Kaiser UB. Mutations in the human gonadotropin-releasing hormone receptor: insights into receptor biology and function. Semin. Reprod. Med. 2007;25:368–378. - PubMed
-
- Bouligand J, Ghervan C, Tello JA, Brailly-Tabard S, Salenave S, Chanson P, Lombes M, Millar RP, Guiochon-Mantel A, Young J. Isolated familial hypogonadotropic hypogonadism and a GNRH1 mutation. N Engl J Med. 2009;360:2742–2748. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
