

Perineural dexmedetomidine added to ropivacaine for sciatic nerve block in rats prolongs the duration of analgesia by blocking the hyperpolarization-activated cation current
- PMID: 21666435
- PMCID: PMC3179561
- DOI: 10.1097/ALN.0b013e318221fcc9
Perineural dexmedetomidine added to ropivacaine for sciatic nerve block in rats prolongs the duration of analgesia by blocking the hyperpolarization-activated cation current
Abstract
Background: The current study was designed to test the hypothesis that the increased duration of analgesia caused by adding dexmedetomidine to local anesthetic results from blockade of the hyperpolarization-activated cation (I(h)) current.
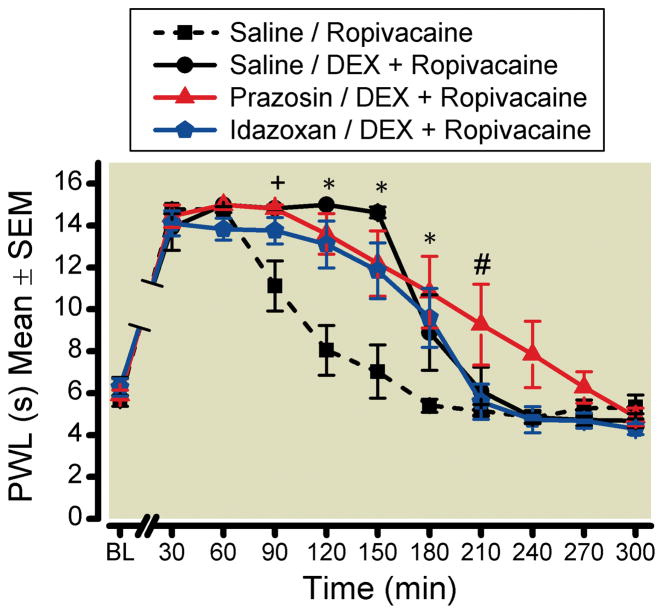
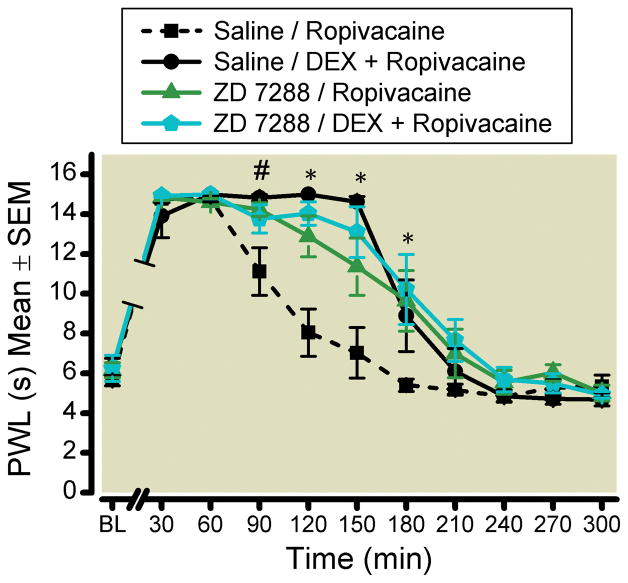
Methods: In this randomized, blinded, controlled study, the analgesic effects of peripheral nerve blocks using 0.5% ropivacaine alone or 0.5% ropivacaine plus dexmedetomidine (34 μM or 6 μg/kg) were assessed with or without the pretreatment of α(1)- and α(2)-adrenoceptor antagonists (prazosin and idazoxan, respectively) and antagonists and agonists of the I(h) current (ZD 7288 and forskolin, respectively). Sciatic nerve blocks were performed, and analgesia was measured by paw withdrawal latency to a thermal stimulus every 30 min for 300 min postblock.
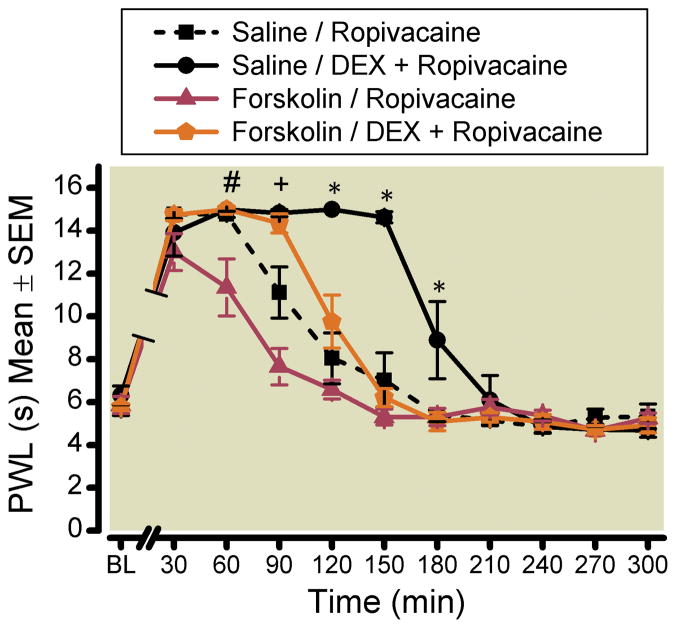
Results: The analgesic effect of dexmedetomidine added to ropivacaine was not reversed by either prazosin or idazoxan. There were no additive or attenuated effects from the pretreatment with ZD 7288 (I(h) current blocker) compared with dexmedetomidine added to ropivacaine. When forskolin was administered as a pretreatment to ropivacaine plus dexmedetomidine, there were statistically significant reductions in duration of analgesia at time points 90-180 min (P < 0.0001 for each individual comparison). The duration of blockade for the forskolin (768 μM) followed by ropivacaine plus dexmedetomidine group mirrored the pattern of the ropivacaine alone group, thereby implying a reversal effect.
Conclusion: Dexmedetomidine added to ropivacaine caused approximately a 75% increase in the duration of analgesia, which was reversed by pretreatment with an I(h) current enhancer. The analgesic effect of dexmedetomidine was not reversed by an α(2)-adrenoceptor antagonist.
Figures
References
-
- Casati A, Fanelli G, Albertin A, Deni F, Anelati D, Antonino FA, Beccaria P. Interscalene brachial plexus anesthesia with either 0.5% ropivacaine or 0.5% bupivacaine. Minerva Anestesiol. 2000;66:39–44. - PubMed
-
- Casati A, Fanelli G, Aldegheri G, Berti M, Colnaghi E, Cedrati V, Torri G. Interscalene brachial plexus anaesthesia with 0.5%, 0.75% or 1% ropivacaine: A double-blind comparison with 2% mepivacaine. Br J Anaesth. 1999;83:872–5. - PubMed
-
- Apfelbaum JL, Gan TJ, Zhao S, Hanna DB, Chen C. Reliability and validity of the perioperative opioid-related symptom distress scale. Anesth Analg. 2004;99:699–709. - PubMed
-
- Lydic R, Baghdoyan HA. In: Neurochemical mechanisms mediating opioid-induced REM sleep disruption, Sleep and Pain. Lavigne G, Sessle BJ, Choiniere M, Soja PJ, editors. Seattle: International Association for the Study of Pain (IASP) Press; 2007. pp. 99–122.
-
- Brummett CM, Amodeo FS, Janda AM, Padda AK, Lydic R. Perineural dexmedetomidine provides an increased duration of analgesia to a thermal stimulus when compared with a systemic control in a rat sciatic nerve block. Reg Anesth Pain Med. 2010;35:427–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
