

Diagnosis and management of pericardial effusion
- PMID: 21666814
- PMCID: PMC3110902
- DOI: 10.4330/wjc.v3.i5.135
Diagnosis and management of pericardial effusion
Abstract
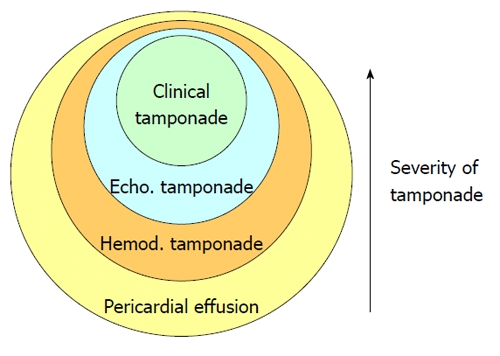
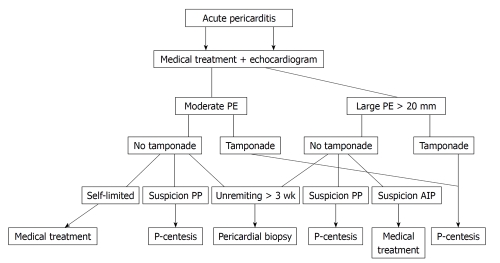
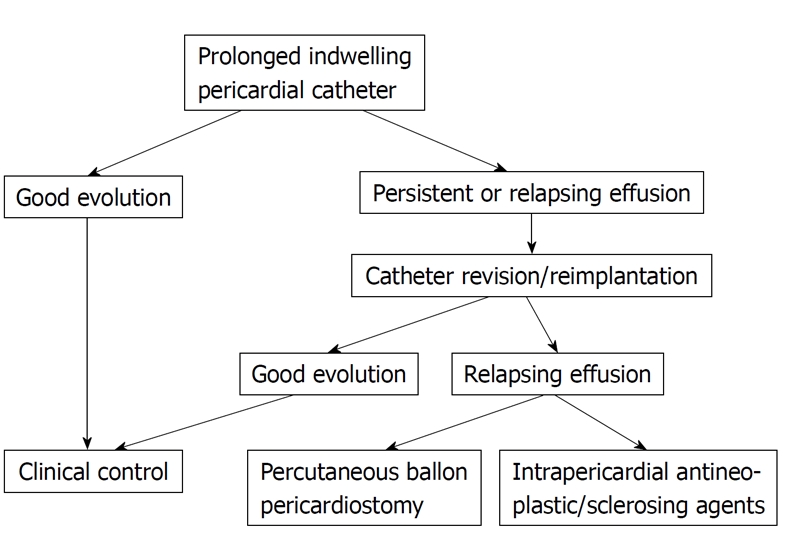
Pericardial effusion is a common finding in everyday clinical practice. The first challenge to the clinician is to try to establish an etiologic diagnosis. Sometimes, the pericardial effusion can be easily related to a known underlying disease, such as acute myocardial infarction, cardiac surgery, end-stage renal disease or widespread metastatic neoplasm. When no obvious cause is apparent, some clinical findings can be useful to establish a diagnosis of probability. The presence of acute inflammatory signs (chest pain, fever, pericardial friction rub) is predictive for acute idiopathic pericarditis irrespective of the size of the effusion or the presence or absence of tamponade. Severe effusion with absence of inflammatory signs and absence of tamponade is predictive for chronic idiopathic pericardial effusion, and tamponade without inflammatory signs for neoplastic pericardial effusion. Epidemiologic considerations are very important, as in developed countries acute idiopathic pericarditis and idiopathic pericardial effusion are the most common etiologies, but in some underdeveloped geographic areas tuberculous pericarditis is the leading cause of pericardial effusion. The second point is the evaluation of the hemodynamic compromise caused by pericardial fluid. Cardiac tamponade is not an "all or none" phenomenon, but a syndrome with a continuum of severity ranging from an asymptomatic elevation of intrapericardial pressure detectable only through hemodynamic methods to a clinical tamponade recognized by the presence of dyspnea, tachycardia, jugular venous distension, pulsus paradoxus and in the more severe cases arterial hypotension and shock. In the middle, echocardiographic tamponade is recognized by the presence of cardiac chamber collapses and characteristic alterations in respiratory variations of mitral and tricuspid flow. Medical treatment of pericardial effusion is mainly dictated by the presence of inflammatory signs and by the underlying disease if present. Pericardial drainage is mandatory when clinical tamponade is present. In the absence of clinical tamponade, examination of the pericardial fluid is indicated when there is a clinical suspicion of purulent pericarditis and in patients with underlying neoplasia. Patients with chronic massive idiopathic pericardial effusion should also be submitted to pericardial drainage because of the risk of developing unexpected tamponade. The selection of the pericardial drainage procedure depends on the etiology of the effusion. Simple pericardiocentesis is usually sufficient in patients with acute idiopathic or viral pericarditis. Purulent pericarditis should be drained surgically, usually through subxiphoid pericardiotomy. Neoplastic pericardial effusion constitutes a more difficult challenge because reaccumulation of pericardial fluid is a concern. The therapeutic possibilities include extended indwelling pericardial catheter, percutaneous pericardiostomy and intrapericardial instillation of antineoplastic and sclerosing agents. Massive chronic idiopathic pericardial effusions do not respond to medical treatment and tend to recur after pericardiocentesis, so wide anterior pericardiectomy is finally necessary in many cases.
Keywords: Diagnosis; Etiology; Pericardial effusion; Therapy.
Figures
References
-
- Savage DD, Garrison RJ, Brand F, Anderson SJ, Castelli WP, Kannel WB, Feinleib M. Prevalence and correlates of posterior extra echocardiographic spaces in a free-living population based sample (the Framingham study) Am J Cardiol. 1983;51:1207–1212. - PubMed
-
- Restrepo CS, Lemos DF, Lemos JA, Velasquez E, Diethelm L, Ovella TA, Martinez S, Carrillo J, Moncada R, Klein JS. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007;27:1595–1610. - PubMed
-
- Galve E, Garcia-Del-Castillo H, Evangelista A, Batlle J, Permanyer-Miralda G, Soler-Soler J. Pericardial effusion in the course of myocardial infarction: incidence, natural history, and clinical relevance. Circulation. 1986;73:294–299. - PubMed
-
- Figueras J, Juncal A, Carballo J, Cortadellas J, Soler JS. Nature and progression of pericardial effusion in patients with a first myocardial infarction: relationship to age and free wall rupture. Am Heart J. 2002;144:251–258. - PubMed
-
- Posner MR, Cohen GI, Skarin AT. Pericardial disease in patients with cancer. The differentiation of malignant from idiopathic and radiation-induced pericarditis. Am J Med. 1981;71:407–413. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
