

Role of procalcitonin and C-reactive protein in differentiation of mixed bacterial infection from 2009 H1N1 viral pneumonia
- PMID: 21668682
- PMCID: PMC5780656
- DOI: 10.1111/j.1750-2659.2011.00244.x
Role of procalcitonin and C-reactive protein in differentiation of mixed bacterial infection from 2009 H1N1 viral pneumonia
Abstract
Background: Mixed bacterial infection is an important contributor to morbidity and mortality during influenza pandemics. We evaluated procalcitonin (PCT) and C-reactive protein (CRP) in differentiating pneumonia caused by mixed bacterial and 2009 H1N1 influenza infection from 2009 H1N1 influenza infection alone.
Methods: Data were collected retrospectively over a 7-month period during the 2009 H1N1 influenza pandemic. Patients visiting emergency department and diagnosed as community-acquired pneumonia caused by 2009 H1N1 infection were included (n = 60).
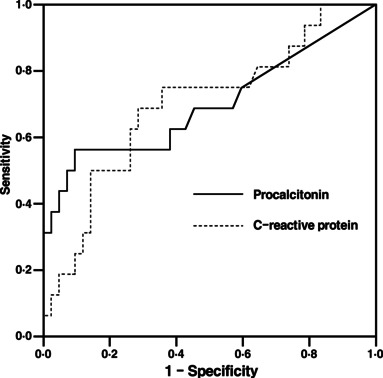
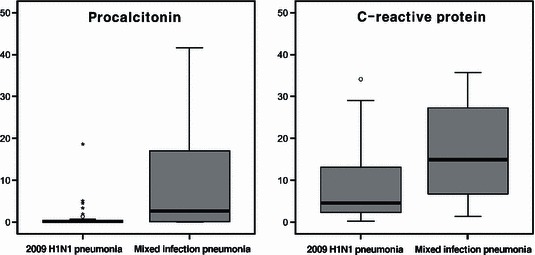
Results: Mixed bacterial and viral infection pneumonia (n = 16) had significantly higher PCT and CRP levels than pneumonia caused by 2009 H1N1 influenza alone (n = 44, P = 0·019, 0·022 respectively). The sensitivity and specificity for detection of mixed bacterial infection pneumonia was 56% and 84% for PCT > 1·5 ng/ml, and 69% and 63% for CRP > 10 mg/dl. Using PCT and CRP in combination, the sensitivity and specificity were 50% and 93%, respectively.
Conclusion: Procalcitonin and CRP alone and their combination had a moderate ability to detect pneumonia of mixed bacterial infection during the 2009 H1N1 pandemic. Considering high specificity, combination of low CRP and PCT result may suggest that pneumonia is unlikely to be caused by mixed bacterial infection.
© 2011 Blackwell Publishing Ltd.
Figures
References
-
- Perez‐Padilla R, de la Rosa‐Zamboni D, Ponce de Leon S et al. Pneumonia and respiratory failure from swine‐origin influenza A (H1N1) in Mexico. N Engl J Med 2009; 361:680–689. - PubMed
-
- WHO . Pandemic (H1N1) 2009 – update 87. Available at http://www.who.int/csr/don/2010_02_12/en/index.html (Accessed 18 February 2010).
-
- Thompson WW, Shay DK, Weintraub E et al. Influenza‐associated hospitalizations in the United States. JAMA 2004; 292:1333–1340. - PubMed
-
- Thompson WW, Shay DK, Weintraub E et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 2003; 289:179–186. - PubMed
-
- Choi WJ, Kim WY, Kim SH et al. Clinical characteristics of pneumonia in hospitalized patients with novel influenza A (H1N1) in Korea. Scand J Infect Dis 2010; 42:311–314. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
