

Discrimination of individuals in a general population at high-risk for alcoholic and non-alcoholic fatty liver disease based on liver stiffness: a cross section study
- PMID: 21669003
- PMCID: PMC3154156
- DOI: 10.1186/1471-230X-11-70
Discrimination of individuals in a general population at high-risk for alcoholic and non-alcoholic fatty liver disease based on liver stiffness: a cross section study
Abstract
Background: Factors associated with liver stiffness (LS) are unknown and normal reference values for LS have not been established. Individuals at high risk for alcoholic (ALD) and non-alcoholic fatty (NAFLD) liver disease need to be non-invasively discriminated during routine health checks. Factors related to LS measured using a FibroScan and normal reference values for LS are presented in this report.
Methods: We measured LS using a FibroScan in 416 consecutive individuals who presented for routine medical checks. We also investigated the relationship between LS and age, body mass index (BMI), liver function (LF), alcohol consumption, and fatty liver determined by ultrasonography. We identified individuals at high-risk for ALD and NAFLD as having a higher LS value than the normal upper limit detected in 171 healthy controls.
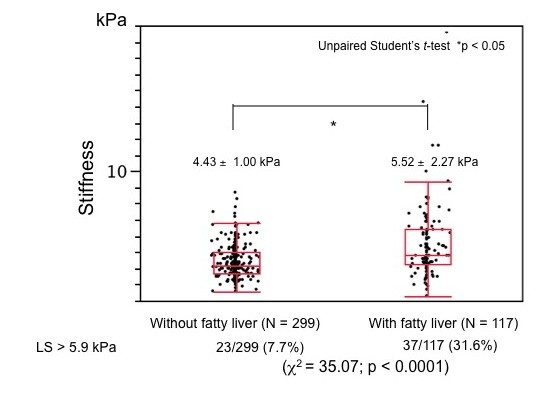
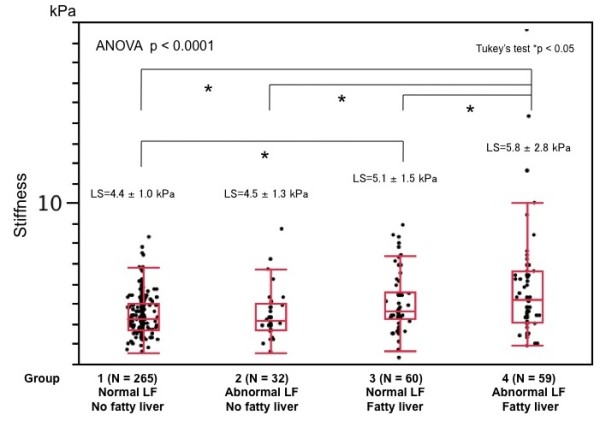
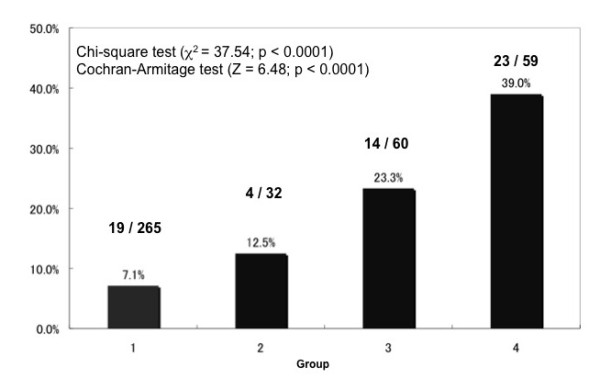
Results: The LS value for all individuals was 4.7 +/- 1.5 kPa (mean +/- SD) and LS significantly and positively correlated with BMI and LF test results. The LS was significantly higher among individuals with, than without fatty liver. Liver stiffness in the 171 healthy controls was 4.3 +/- 0.81 kPa and the upper limit of LS in the normal controls was 5.9 kPa. We found that 60 (14.3%) of 416 study participants had abnormal LS. The proportion of individuals whose LS values exceeded the normal upper limit was over five-fold higher among those with, than without fatty liver accompanied by abnormal LF test results.
Conclusions: Liver stiffness could be used to non-invasively monitor the progression of chronic liver diseases and to discriminate individuals at high risk for ALD and NAFLD during routine health assessments.
Figures




References
-
- Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology. 2003;38:1449–57. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
