

Management of severe sepsis in patients admitted to Asian intensive care units: prospective cohort study
- PMID: 21669950
- PMCID: PMC3113333
- DOI: 10.1136/bmj.d3245
Management of severe sepsis in patients admitted to Asian intensive care units: prospective cohort study
Abstract
Objectives: To assess the compliance of Asian intensive care units and hospitals to the Surviving Sepsis Campaign's resuscitation and management bundles. Secondary objectives were to evaluate the impact of compliance on mortality and the organisational characteristics of hospitals that were associated with higher compliance.
Design: Prospective cohort study.
Setting: 150 intensive care units in 16 Asian countries.
Participants: 1285 adult patients with severe sepsis admitted to these intensive care units in July 2009. The organisational characteristics of participating centres, the patients' baseline characteristics, the achievement of targets within the resuscitation and management bundles, and outcome data were recorded.
Main outcome measure: Compliance with the Surviving Sepsis Campaign's resuscitation (six hours) and management (24 hours) bundles.
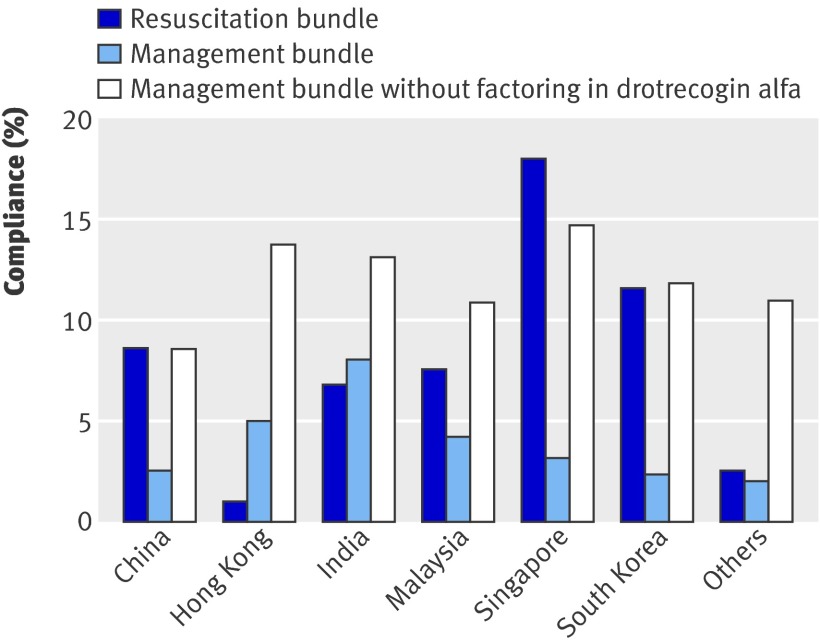
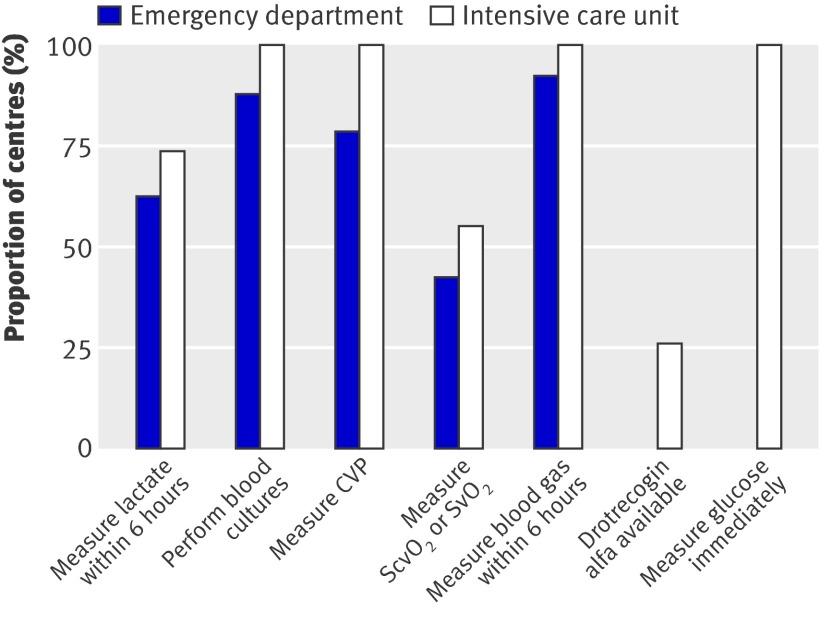
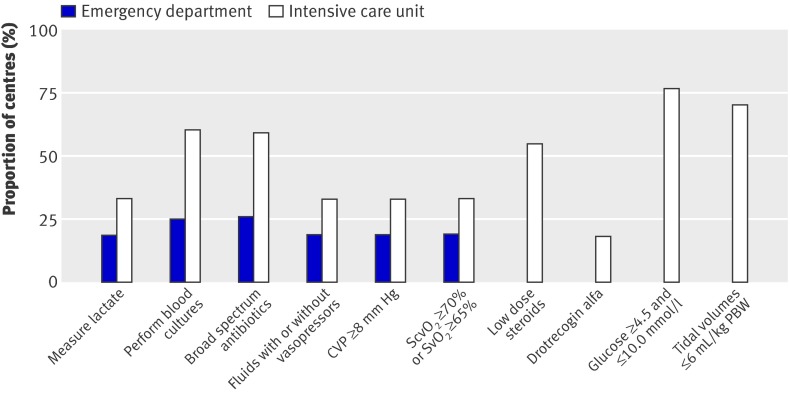
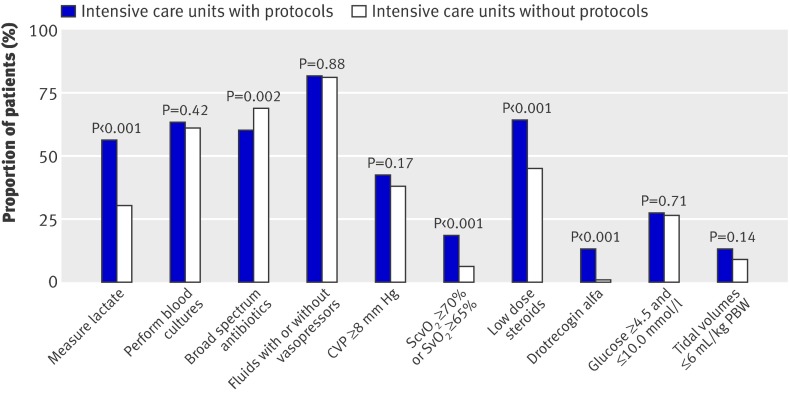
Results: Hospital mortality was 44.5% (572/1285). Compliance rates for the resuscitation and management bundles were 7.6% (98/1285) and 3.5% (45/1285), respectively. On logistic regression analysis, compliance with the following bundle targets independently predicted decreased mortality: blood cultures (achieved in 803/1285; 62.5%, 95% confidence interval 59.8% to 65.1%), broad spectrum antibiotics (achieved in 821/1285; 63.9%, 61.3% to 66.5%), and central venous pressure (achieved in 345/870; 39.7%, 36.4% to 42.9%). High income countries, university hospitals, intensive care units with an accredited fellowship programme, and surgical intensive care units were more likely to be compliant with the resuscitation bundle.
Conclusions: While mortality from severe sepsis is high, compliance with resuscitation and management bundles is generally poor in much of Asia. As the centres included in this study might not be fully representative, achievement rates reported might overestimate the true degree of compliance with recommended care and should be interpreted with caution. Achievement of targets for blood cultures, antibiotics, and central venous pressure was independently associated with improved survival.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303-10. - PubMed
-
- Surviving Sepsis Campaign. 2011. www.survivingsepsis.org/Pages/default.aspx.
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006;34:1589-96. - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001;345:1368-77. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical