

Cardiac dysfunction and noncardiac dysfunction as precursors of heart failure with reduced and preserved ejection fraction in the community
- PMID: 21670229
- PMCID: PMC3257876
- DOI: 10.1161/CIRCULATIONAHA.110.979203
Cardiac dysfunction and noncardiac dysfunction as precursors of heart failure with reduced and preserved ejection fraction in the community
Erratum in
- Circulation. 2011 Oct 25;124(17):e458
Abstract
Background: Heart failure (HF) is a clinical syndrome characterized by signs and symptoms involving multiple organ systems. Longitudinal data demonstrating that asymptomatic cardiac dysfunction precedes overt HF are scarce, and the contribution of noncardiac dysfunction to HF progression is unclear. We hypothesized that subclinical cardiac and noncardiac organ dysfunction would accelerate the manifestation of HF.
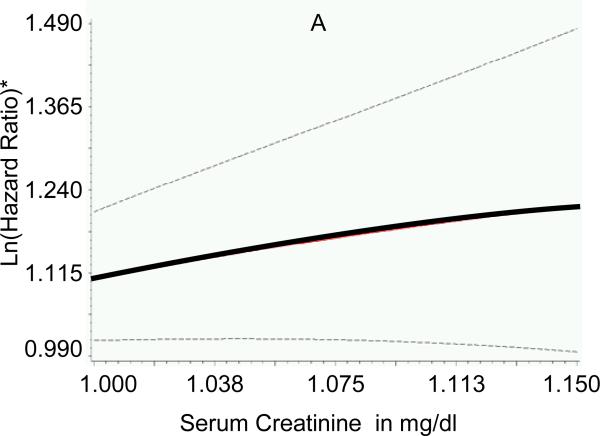
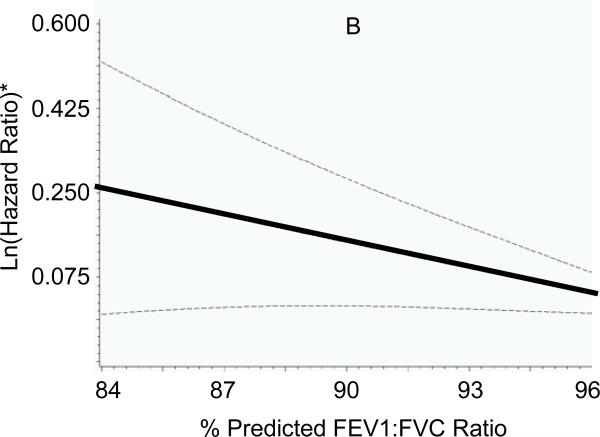
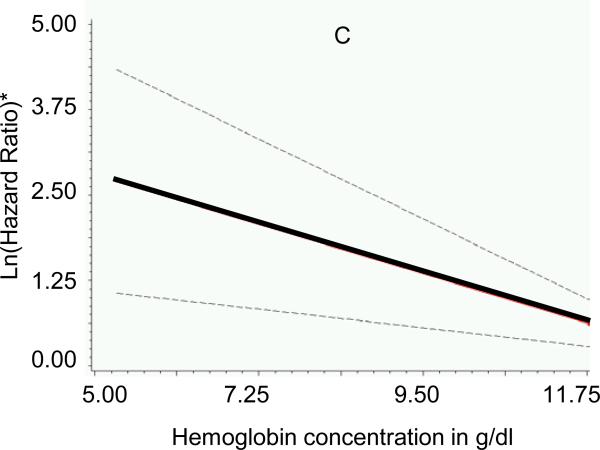
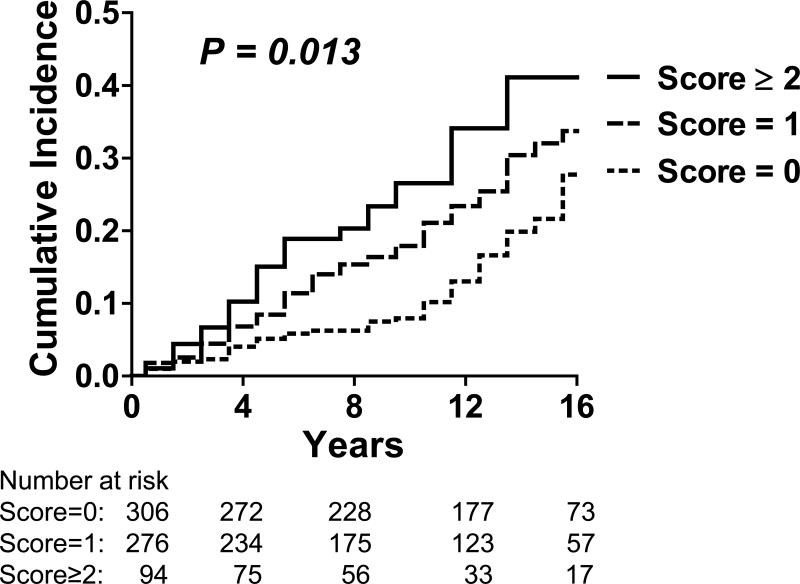
Methods and results: We studied 1038 participants of the Framingham Heart Study original cohort (mean age, 76±5 years; 39% men) with routine assessment of left ventricular systolic and diastolic function. Major noncardiac organ systems were assessed with the use of serum creatinine (renal), serum albumin (hepatic), ratio of forced expiratory volume in 1 second to forced vital capacity (FEV(1):FVC ratio; pulmonary), hemoglobin concentration (hematologic/oxygen-carrying capacity), and white blood cell count (systemic inflammation). On follow-up (mean, 11 years), there were 248 incident HF events (146 in women). After adjustment for established HF risk factors, antecedent left ventricular systolic dysfunction (hazard ratio, 2.33; 95% confidence interval, 1.43 to 3.78) and diastolic dysfunction (hazard ratio, 1.32; 95% confidence interval, 1.01 to 1.71) were associated with increased HF risk. After adjustment for cardiac dysfunction, higher serum creatinine, lower FEV1:FVC ratios, and lower hemoglobin concentrations were associated with increased HF risk (all P<0.05); serum albumin and white blood cell count were not. Subclinical dysfunction in each noncardiac organ system was associated with a 30% increased risk of HF (P=0.013).
Conclusions: Antecedent cardiac dysfunction and noncardiac organ dysfunction are associated with increased incidence of HF, supporting the notion that HF is a progressive syndrome and underscoring the importance of noncardiac factors in its occurrence.
Figures
Comment in
-
Omnes viae Romam ducunt: Asymptomatic cardiac and noncardiac organ system dysfunction leads to heart failure.Circulation. 2011 Jul 5;124(1):4-6. doi: 10.1161/CIRCULATIONAHA.111.035287. Circulation. 2011. PMID: 21730317 No abstract available.
References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391–479. - PubMed
-
- Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, Tavazzi L, Smiseth OA, Gavazzi A, Haverich A, Hoes A, Jaarsma T, Korewicki J, Levy S, Linde C, Lopez-Sendon JL, Nieminen MS, Pierard L, Remme WJ. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115–1140. - PubMed
-
- Redfield MM, Jacobsen SJ, Burnett JC, Jr., Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. - PubMed
-
- Smith GL, Shlipak MG, Havranek EP, Foody JM, Masoudi FA, Rathore SS, Krumholz HM. Serum urea nitrogen, creatinine, and estimators of renal function: mortality in older patients with cardiovascular disease. Arch Intern Med. 2006;166:1134–1142. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
