

High mean fluorescence intensity donor-specific anti-HLA antibodies associated with chronic rejection Postliver transplant
- PMID: 21672151
- PMCID: PMC4412604
- DOI: 10.1111/j.1600-6143.2011.03593.x
High mean fluorescence intensity donor-specific anti-HLA antibodies associated with chronic rejection Postliver transplant
Abstract
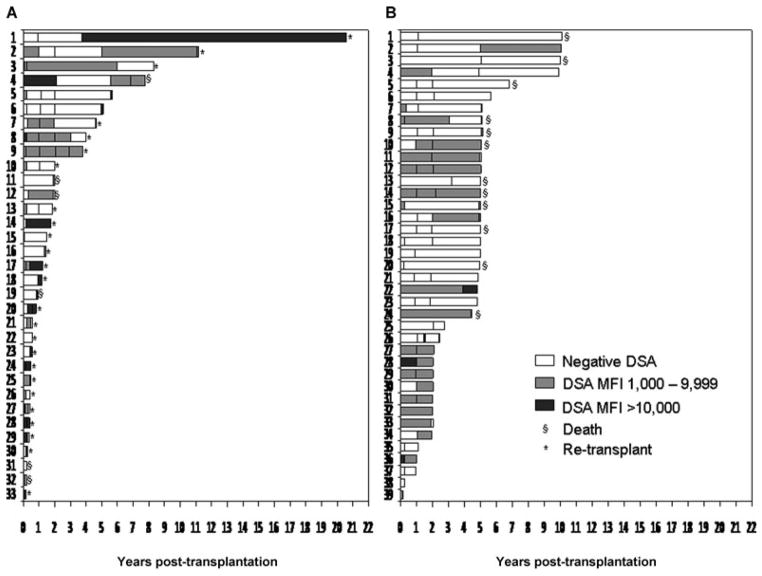
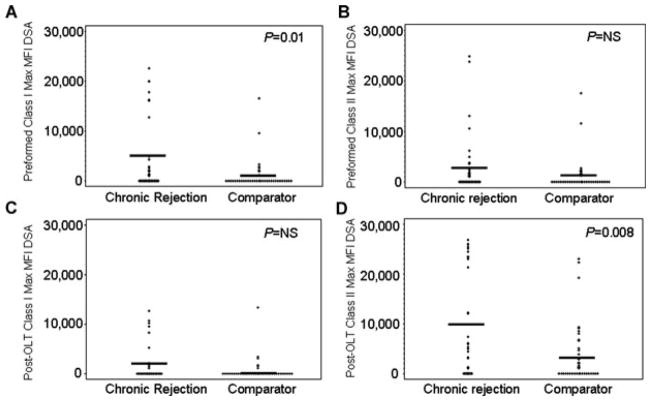
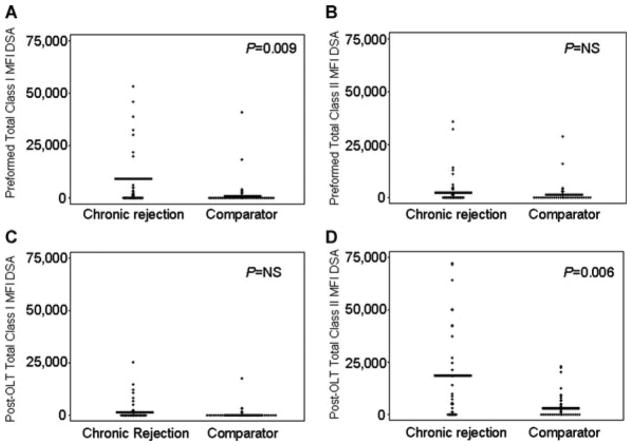
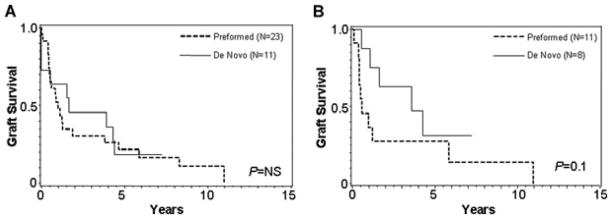
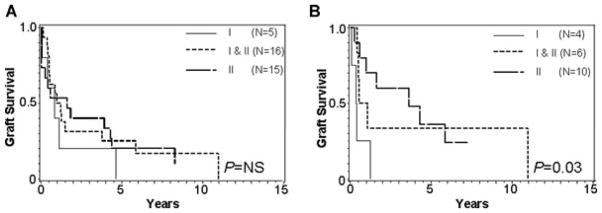
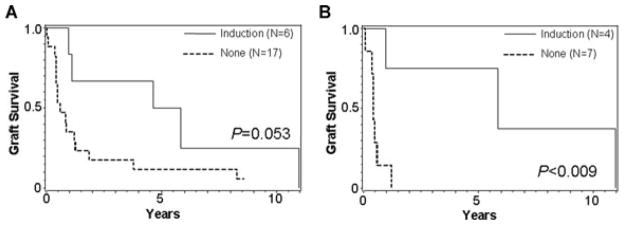
In contrast to kidney transplantation where donor-specific anti-HLA antibodies (DSA) negatively impact graft survival, correlation of DSA with clinical outcomes in patients after orthotopic liver transplantation (OLT) has not been clearly established. We hypothesized that DSA are present in patients who develop chronic rejection after OLT. Prospectively collected serial serum samples on 39 primary OLT patients with biopsy-proven chronic rejection and 39 comparator patients were blinded and analyzed for DSA using LABScreen(®) single antigen beads test, where a 1000 mean fluorescence value was considered positive. In study patients, the median graft survival was 15 months, 74% received ≥ one retransplant, 20% remain alive and 87% had ≥ one episode of acute rejection. This is in contrast to comparator patients where 69% remain alive, and no patient needed retransplant or experienced rejection. Thirty-six chronic rejection patients (92%) and 24 (61%) comparator patients had DSA (p = 0.003). Chronic rejection versus comparator patients had higher mean fluorescence intensity (MFI) DSA. Although a further study with larger numbers of patients is needed to identify clinically significant thresholds, there is an association of high-MFI DSA with chronic rejection after OLT.
© 2011 The Authors Journal compilation © 2011 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
P.I.T.—One Lambda Incorporated Chairman and major share holder. H.K. was a consultant for One Lambda. All the other authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
-
- Moore SB, Wiesner RH, Perkins JD, Nagorney DM, Sterioff S, Krom RA. A positive lymphocyte cross-match and major histo-compatibility complex mismatching do not predict early rejection of liver transplants in patients treated with cyclosporine. Transplant Proc. 1987;19(Pt 3):2390–2391. - PubMed
-
- Ogura K, Koyama H, Takemoto S, Terasaki PI, Busuttil RW. Significance of a positive crossmatch on outcome in human liver transplantation. Transplant Proc. 1992;24:1465. - PubMed
-
- Ogura K, Terasaki PI, Koyama H, Chia J, Imagawa DK, Busuttil RW. High one-month liver graft failure rates in flow cytometry crossmatch-positive recipients. Clin Transplant. 1994;8(Pt1):111–115. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
