

Clarifying differences in natural history between models of screening: the case of colorectal cancer
- PMID: 21673187
- PMCID: PMC3531980
- DOI: 10.1177/0272989X11408915
Clarifying differences in natural history between models of screening: the case of colorectal cancer
Abstract
Background: Microsimulation models are important decision support tools for screening. However, their complexity makes them difficult to understand and limits realization of their full potential. Therefore, it is important to develop documentation that clarifies their structure and assumptions. The authors demonstrate this problem and explore a solution for natural history using 3 independently developed colorectal cancer screening models.
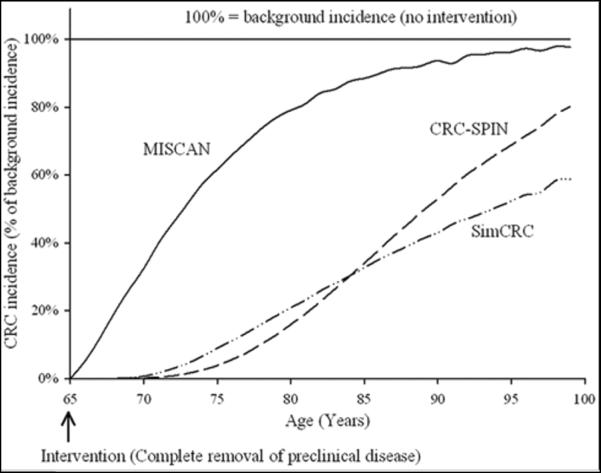
Methods: The authors first project effectiveness and cost-effectiveness of colonoscopy screening for the 3 models (CRC-SPIN, SimCRC, and MISCAN). Next, they provide a conventional presentation of each model, including information on structure and parameter values. Finally, they report the simulated reduction in clinical cancer incidence following a one-time complete removal of adenomas and preclinical cancers for each model. They call this new measure the maximum clinical incidence reduction (MCLIR).
Results: Projected effectiveness varies widely across models. For example, estimated mortality reduction for colonoscopy screening every 10 years from age 50 to 80 years, with surveillance in adenoma patients, ranges from 65% to 92%. Given only conventional information, it is difficult to explain these differences, largely because differences in structure make parameter values incomparable. In contrast, the MCLIR clearly shows the impact of model differences on the key feature of natural history, the dwell time of preclinical disease. Dwell times vary from 8 to 25 years across models and help explain differences in projected screening effectiveness.
Conclusions: The authors propose a new measure, the MCLIR, which summarizes the implications for predicted screening effectiveness of differences in natural history assumptions. Including the MCLIR in the standard description of a screening model would improve the transparency of these models.
Figures
Comment in
-
Exploring the unknown and the unknowable with simulation models.Med Decis Making. 2011 Jul-Aug;31(4):521-3. doi: 10.1177/0272989X11412078. Med Decis Making. 2011. PMID: 21757646 No abstract available.
-
Cross-model comparisons to improve the value of modeling: the case of colorectal cancer screening.Med Decis Making. 2011 Jul-Aug;31(4):524-6. doi: 10.1177/0272989X11412195. Med Decis Making. 2011. PMID: 21757647 No abstract available.
-
Using models to make policy: an inflection point?Med Decis Making. 2011 Jul-Aug;31(4):527-9. doi: 10.1177/0272989X11412079. Med Decis Making. 2011. PMID: 21757648 No abstract available.
References
-
- Song K, Fendrick AM, Ladabaum U. Fecal DNA testing compared with conventional colorectal cancer screening methods: a decision analysis. Gastroenterology. 2004;126(5):1270–9. - PubMed
-
- Pickhardt PJ, Hassan C, Laghi A, Zullo A, Kim DH, Morini S. Cost-effectiveness of colorectal cancer screening with computed tomography colonography: the impact of not reporting diminutive lesions. Cancer. 2007;109(11):2213–21. - PubMed
-
- Vijan S, Hwang EW, Hofer TP, Hayward RA. Which colon cancer screening test? A comparison of costs, effectiveness, and compliance. Am J Med. 2001;111(8):593–601. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
