

Current management of inflammatory bowel disease and colorectal cancer
- PMID: 21673876
- PMCID: PMC3109885
Current management of inflammatory bowel disease and colorectal cancer
Abstract
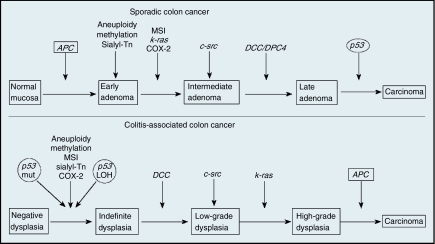
INFLAMMATORY BOWEL DISEASES (IBDS) CAN BE DIVIDED INTO TWO MAJOR DISORDERS: ulcerative colitis and Crohn's disease. Although IBD-associated colorectal cancer (IBD-CRC) accounts for only 1-2% of all cases of colorectal cancer, IBD with colon involvement is among the top three high-risk conditions for colorectal cancer. Today, colorectal cancer accounts for approximately 10-15% of all deaths among IBD patients. Indeed, patients with IBD colitis are six times more likely to develop colorectal cancer than the general population and have a higher frequency of multiple synchronous colorectal cancers. Since IBD-CRC was first described in 1925, the colon remains the primary site of neoplasms in IBD patients today. Ulcerative colitis-associated colorectal cancer is most common in the rectum and sigmoid colon, whereas Crohn's disease-associated colorectal cancer is evenly distributed between the different colon segments. Chemoprevention of colorectal cancer remains an important goal, and colonoscopy surveillance programs are critical to early detection in these patients. Newer methods, such as chromoendoscopy, are currently being investigated as complementary techniques to enhance early detection of dysplasia and cancer in this high-risk population. We present a comprehensive review of the relationship between inflammatory bowel disease and colorectal cancer. Major themes covered include risk factors for IBD-CRC and the molecular pathobiology of progression from dysplasia to cancer, endoscopic surveillance and new methods for early detection of dysplasia, approaches to prevention of IBD-CRC, and current recommendations and controversies regarding the treatment of dysplasia. In particular, disagreement has arisen over optimal management of low-grade dysplasia, with some IBD experts now advocating close colonoscopic surveillance of patients with low-grade dysplasia rather then total colectomy.
Figures

References
-
- Calkins BM, Lilienfeld AM, Garland CF, et al. : Trends in incidence rates of ulcerative colitis and Crohn's disease. Dig Dis Sci 29(10):913–920, 1984 - PubMed
-
- Loftus EV, Jr: Management of extraintestinal manifestations and other complications of inflammatory bowel disease. Curr Gastroenterol Rep 6(6):506–513, 2004 - PubMed
-
- Crohn BB: The sigmoidoscopic picture of chronic ulcerative colitis (non-specific). Amer J Med Sci 170:220–228, 1925
-
- Munkholm P: Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease. Aliment Pharmacol Ther 18(suppl 2):1–5, 2003 - PubMed
-
- Lennard-Jones JE, Ritchie JK, Williams CB: Cancer surveillance in ulcerative colitis: experience over 15 years. Lancet 2:149–152, 1983 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources