

Immunological and cardiometabolic risk factors in the prediction of type 2 diabetes and coronary events: MONICA/KORA Augsburg case-cohort study
- PMID: 21674000
- PMCID: PMC3108947
- DOI: 10.1371/journal.pone.0019852
Immunological and cardiometabolic risk factors in the prediction of type 2 diabetes and coronary events: MONICA/KORA Augsburg case-cohort study
Abstract
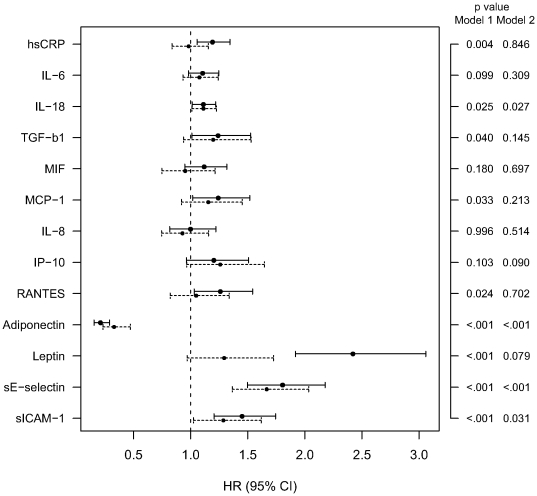
Background: This study compares inflammation-related biomarkers with established cardiometabolic risk factors in the prediction of incident type 2 diabetes and incident coronary events in a prospective case-cohort study within the population-based MONICA/KORA Augsburg cohort.
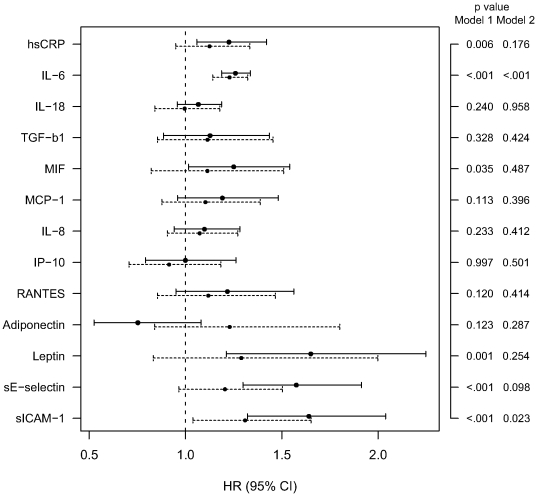
Methods and findings: Analyses for type 2 diabetes are based on 436 individuals with and 1410 individuals without incident diabetes. Analyses for coronary events are based on 314 individuals with and 1659 individuals without incident coronary events. Mean follow-up times were almost 11 years. Areas under the receiver-operating characteristic curve (AUC), changes in Akaike's information criterion (ΔAIC), integrated discrimination improvement (IDI) and net reclassification index (NRI) were calculated for different models. A basic model consisting of age, sex and survey predicted type 2 diabetes with an AUC of 0.690. Addition of 13 inflammation-related biomarkers (CRP, IL-6, IL-18, MIF, MCP-1/CCL2, IL-8/CXCL8, IP-10/CXCL10, adiponectin, leptin, RANTES/CCL5, TGF-β1, sE-selectin, sICAM-1; all measured in nonfasting serum) increased the AUC to 0.801, whereas addition of cardiometabolic risk factors (BMI, systolic blood pressure, ratio total/HDL-cholesterol, smoking, alcohol, physical activity, parental diabetes) increased the AUC to 0.803 (ΔAUC [95% CI] 0.111 [0.092-0.149] and 0.113 [0.093-0.149], respectively, compared to the basic model). The combination of all inflammation-related biomarkers and cardiometabolic risk factors yielded a further increase in AUC to 0.847 (ΔAUC [95% CI] 0.044 [0.028-0.066] compared to the cardiometabolic risk model). Corresponding AUCs for incident coronary events were 0.807, 0.825 (ΔAUC [95% CI] 0.018 [0.013-0.038] compared to the basic model), 0.845 (ΔAUC [95% CI] 0.038 [0.028-0.059] compared to the basic model) and 0.851 (ΔAUC [95% CI] 0.006 [0.003-0.021] compared to the cardiometabolic risk model), respectively.
Conclusions: Inclusion of multiple inflammation-related biomarkers into a basic model and into a model including cardiometabolic risk factors significantly improved the prediction of type 2 diabetes and coronary events, although the improvement was less pronounced for the latter endpoint.
Conflict of interest statement
Figures
References
-
- Kolb H, Mandrup-Poulsen T. An immune origin of type 2 diabetes? Diabetologia. 2005;48:1038–1050. - PubMed
-
- Larsen CM, Faulenbach M, Vaag A, Vølund A, Ehses JA, et al. Interleukin-1-receptor antagonist in type 2 diabetes mellitus. N Engl J Med. 2007;356:1517–1526. - PubMed
-
- Sattar N, Wannamethee SG, Forouhi NG. Novel biochemical risk factors for type 2 diabetes: pathogenic insights or prediction possibilities? Diabetologia. 2008;51:926–940. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
