

Paradoxical motion in L5-S1 adult spondylolytic spondylolisthesis
- PMID: 21674210
- PMCID: PMC3265596
- DOI: 10.1007/s00586-011-1880-9
Paradoxical motion in L5-S1 adult spondylolytic spondylolisthesis
Abstract
Introduction: In patients with spondylolisthesis, it is assumed that flexion accentuates anterior displacement, whereas extension causes some reduction. Paradoxical movement-where flexion causes reduction of spondylolisthesis and extension increases the anterior translation, is rarely described. In this study, we investigate the prevalence of paradoxical motion in patients with L5-S1 spondylolytic spondylolisthesis and why this abnormal motion occurs.
Materials and methods: Flexion and extension radiographs of 41 patients with grade I and II spondylolytic spondylolisthesis of the L5-S1 segment were analysed. Patients who had previous lumbar spine surgery, recent lumbar spine trauma, those more than 50 years of age and those with poor quality radiographs were excluded.
Results: There were 24 male and 17 female patients. The average age was 32.7 years. Of the 41 patients, 29 (70.7%) showed no significant instability. Six (15%) patients showed anterolisthesis, where flexion accentuated the forward displacement, while further six (15%) patients showed paradoxical motion. Statistical analyses found that patients with paradoxical motion had a significantly higher slip angle.
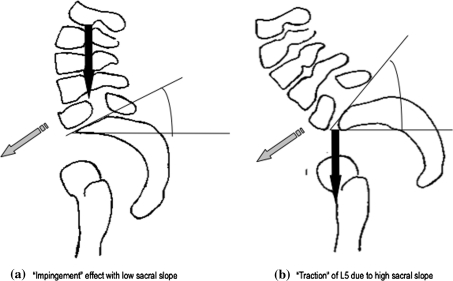
Conclusion: In this study, we have demonstrated that: (1) paradoxical motion in spondylolytic spondylolisthesis is more common than previously thought. (2) Patients without anterolisthesis during flexion in dynamic radiographs may still have (paradoxical) instability. (3) Paradoxical motion may be more common in patients with a low sacral slope and increased lumbosacral lordosis.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
