

Infrastructure to support ultra high throughput biodosimetry screening after a radiological event
- PMID: 21675819
- PMCID: PMC3169379
- DOI: 10.3109/09553002.2011.583317
Infrastructure to support ultra high throughput biodosimetry screening after a radiological event
Abstract
Purpose: After a large-scale radiological event, there will be a pressing need to assess, within a few days, the radiation doses received by tens or hundreds of thousands of individuals. This is for triage, to prevent treatment locations from being overwhelmed, in what is sure to be a resource limited scenario, as well as to facilitate dose-dependent treatment decisions. In addition there are psycho-social considerations, in that active reassurance of minimal exposure is a potentially effective antidote to mass panic, as well as long-term considerations, to facilitate later studies of cancer and other long-term disease risks.
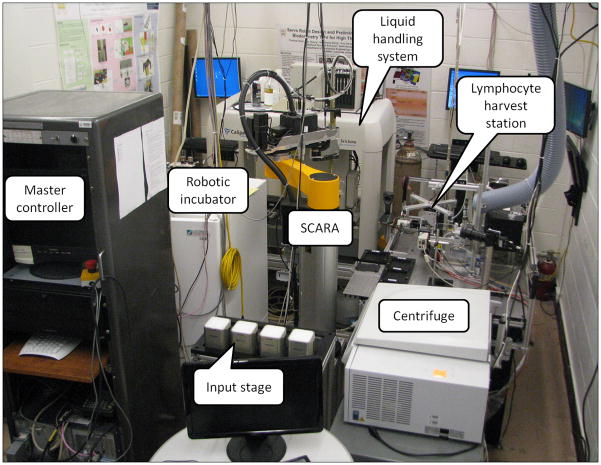
Materials and methods: As described elsewhere in this issue, we are developing a Rapid Automated Biodosimetry Tool (RABiT). The RABiT allows high throughput analysis of thousands of blood samples per day, providing a dose estimate that can be used to support clinical triage and treatment decisions.
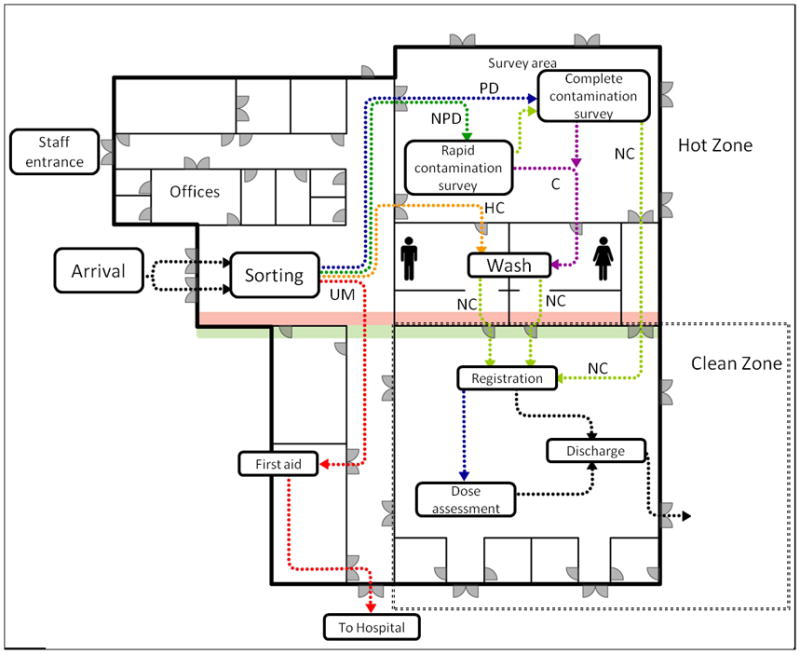
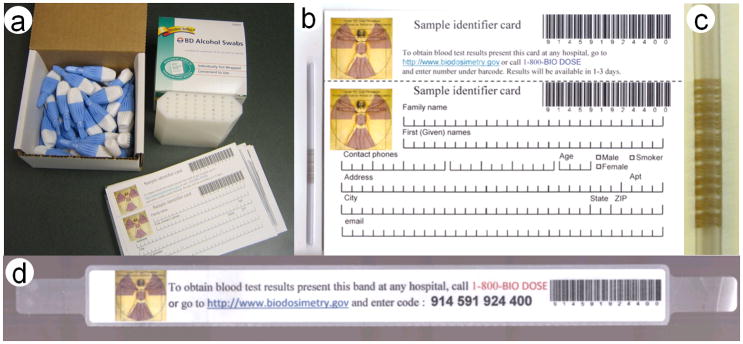
Results: Development of the RABiT has motivated us to consider the logistics of incorporating such a system into the existing emergency response scenarios of a large metropolitan area. We present here a view of how one or more centralized biodosimetry readout devices might be incorporated into an infrastructure in which fingerstick blood samples are taken at many distributed locations within an affected city or region and transported to centralized locations.
Conclusions: High throughput biodosimetry systems offer the opportunity to perform biodosimetric assessments on a large number of persons. As such systems reach a high level of maturity, emergency response scenarios will need to be tweaked to make use of these powerful tools. This can be done relatively easily within the framework of current scenarios.
Conflict of interest statement
The authors report no conflicts of interest.
The content is solely the responsibility of the authors and does not necessarily represent the official views of National Institute of Allergy and Infectious Diseases, the National Institutes of Health or the New York City Department of Health and Mental Hygiene. The concepts discussed here do not necessarily reflect current planning for emergency response at local or national levels.
Figures
References
-
- Aakko E, Weed N, Konrad R, Wiesman J. Rethinking volunteer management using a centralized volunteer staging and training area. Disaster Medicine & Public Health Preparedness. 2008;2:127–129. - PubMed
-
- Amundson SA, Bittner M, Meltzer P, Trent J, Fornace AJJ. Biological indicators for the identification of ionizing radiation exposure in humans. Expert Review of Molecular Diagnostics. 2001;1:211–219. - PubMed
-
- Anno GH, Young RW, Bloom RM, Mercier JR. Dose response relationships for acute ionizing-radiation lethality. Health Physics. 2003;84:565–575. - PubMed
-
- Beaupain B, Leblanc T, Reman O, Hermine O, Vannier JP, Suarez F, Lutz P, Bordigoni P, Jourdain A, Schoenvald M, Ouachee M, Francois S, Kohser F, Jardin F, Devouassoux G, Bertrand Y, Nove-Josserand R, Donadieu J. Is pegfilgrastim safe and effective in congenital neutropenia? An analysis of the french severe chronic neutropenia registry. Pediatric Blood Cancer. 2009;53:1068–1073. - PubMed
-
- Blakely WF, Carr Z, Chu MC, Dayal-Drager R, Fujimoto K, Hopmeir M, Kulka U, Lillis-Hearne P, Livingston G, Lloyd DC, Maznyk N, Perez Mdel R, Romm H, Takashima Y, Voisin P, Wilkins RC, Yoshida MA. Who 1st consultation on the development of a global biodosimetry laboratories network for radiation emergencies (BioDoseNet) Radiation Research. 2009;171:127–139. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials