

An economic history of Medicare part C
- PMID: 21676024
- PMCID: PMC3117270
- DOI: 10.1111/j.1468-0009.2011.00629.x
An economic history of Medicare part C
Erratum in
- Milbank Q. 2013 Mar;91(1):210
Abstract
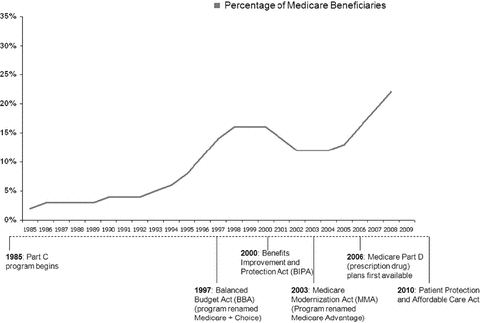
Context: Twenty-five years ago, private insurance plans were introduced into the Medicare program with the stated dual aims of (1) giving beneficiaries a choice of health insurance plans beyond the fee-for-service Medicare program and (2) transferring to the Medicare program the efficiencies and cost savings achieved by managed care in the private sector.
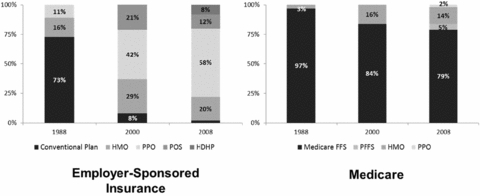
Methods: In this article we review the economic history of Medicare Part C, known today as Medicare Advantage, focusing on the impact of major changes in the program's structure and of plan payment methods on trends in the availability of private plans, plan enrollment, and Medicare spending. Additionally, we compare the experience of Medicare Advantage and of employer-sponsored health insurance with managed care over the same time period.
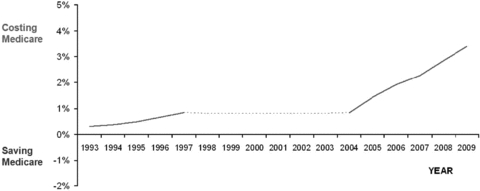
Findings: Beneficiaries' access to private plans has been inconsistent over the program's history, with higher plan payments resulting in greater choice and enrollment and vice versa. But Medicare Advantage generally has cost more than the traditional Medicare program, an overpayment that has increased in recent years.
Conclusions: Major changes in Medicare Advantage's payment rules are needed in order to simultaneously encourage the participation of private plans, the provision of high-quality care, and to save Medicare money.
© 2011 Milbank Memorial Fund. Published by Wiley Periodicals Inc.
Figures
References
-
- Aaron H, Reischauer R. The Medicare Reform Debate: What Is the Next Step? Health Affairs. 1995;14(4):8–31. - PubMed
-
- Achman L, Gold M. Are the 2004 Payment Increases Helping to Stem Medicare Advantage's Benefit Erosion? The Commonwealth Fund. Commonwealth Fund Publication. 2004 no. 795.
-
- Atherly A. Supplemental Insurance: Medicare's Accidental Stepchild. Medical Care Research and Review. 2001;58(2):131–61. - PubMed
-
- Balsa AI, Cao Z, McGuire TG. Does Managed Health Care Reduce Health Care Disparities between Minorities and Whites? Journal of Health Economics. 2007;26:1101–21. - PubMed
-
- Barr MS, Foote SM, Krakauer R, Mattingly PH. Lessons for the New CMS Innovation Center from the Medicare Health Support Program. Health Affairs. 2010;29(7):1305–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
