

Preoperative gabapentin for acute post-thoracotomy analgesia: a randomized, double-blinded, active placebo-controlled study
- PMID: 21676165
- PMCID: PMC3200555
- DOI: 10.1111/j.1533-2500.2011.00480.x
Preoperative gabapentin for acute post-thoracotomy analgesia: a randomized, double-blinded, active placebo-controlled study
Abstract
Background: The role of preoperative gabapentin in postoperative pain management is not clear, particularly in patients receiving regional blockade. Patients undergoing thoracotomy benefit from epidural analgesia but still may experience significant postoperative pain. We examined the effect of preoperative gabapentin in thoracotomy patients.
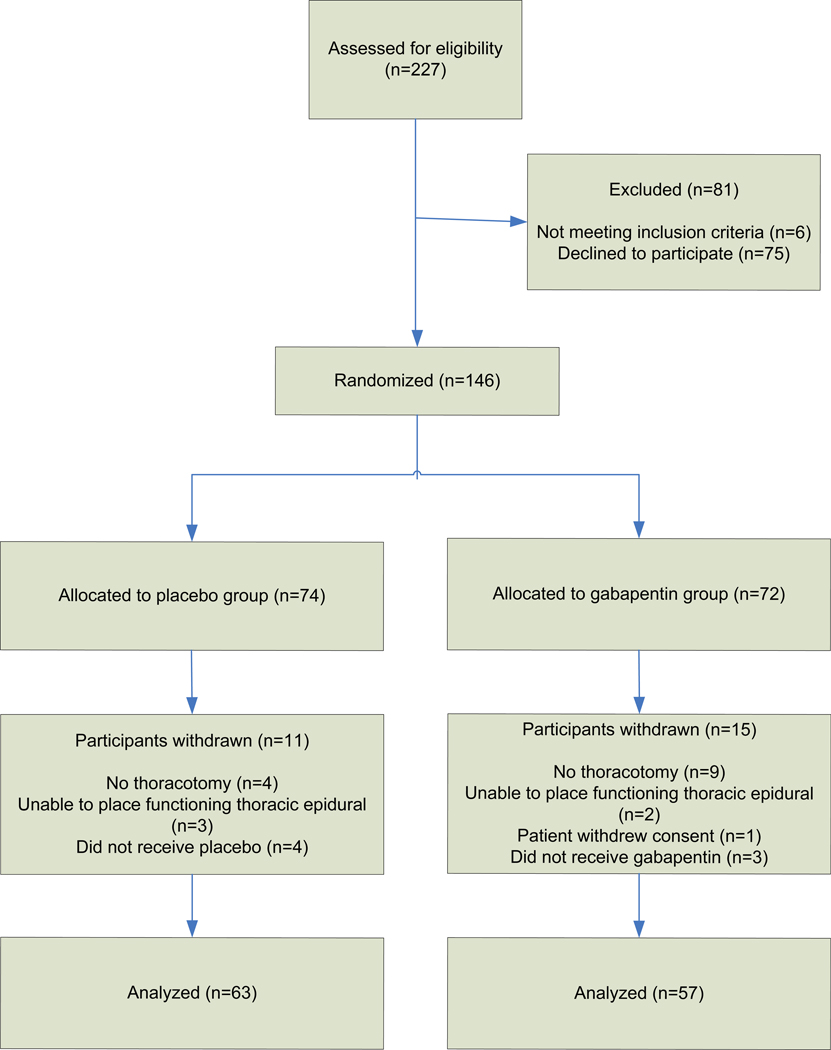
Methods: Adults undergoing elective thoracotomy were enrolled in this prospective, randomized, double-blinded, placebo-controlled study, and randomly assigned to receive 600 mg gabapentin or active placebo (12.5 mg diphenhydramine) orally within 2 hours preoperatively. Standardized management included thoracic epidural infusion, intravenous patient-controlled opioid analgesia, acetaminophen and ketorolac. Pain scores, opioid use and side effects were recorded for 48 hours. Pain was also assessed at 3 months.
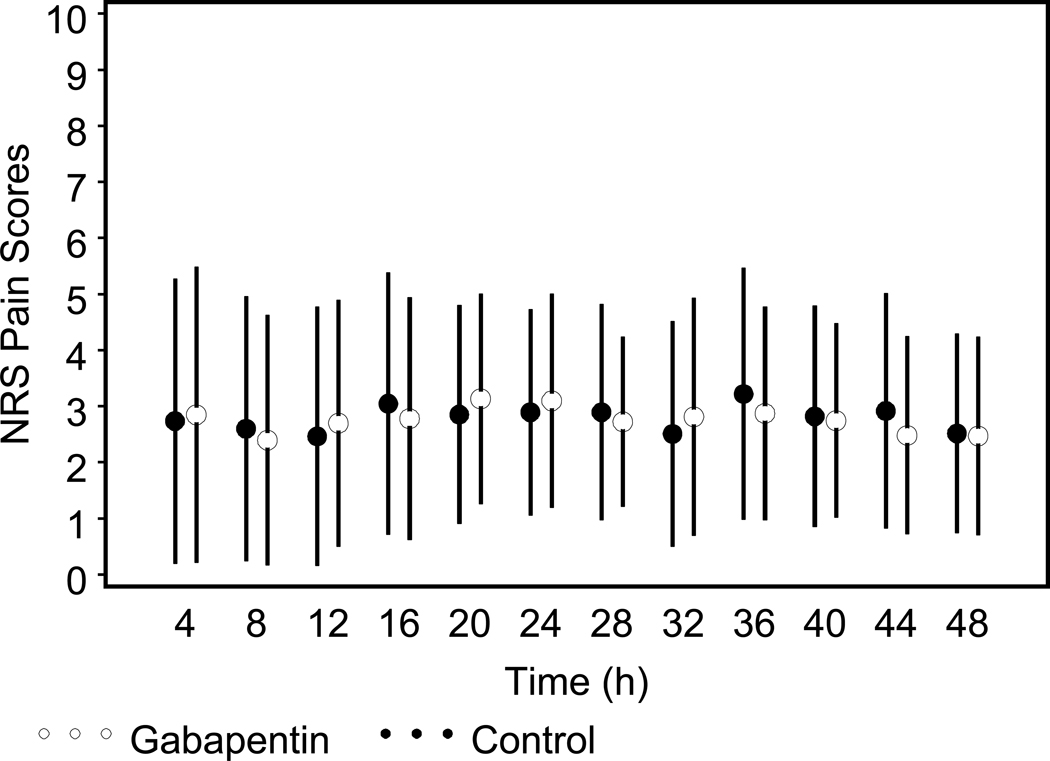
Results: One hundred twenty patients (63 placebo and 57 gabapentin) were studied. Pain scores did not significantly differ at any time point (P = 0.53). Parenteral and oral opioid consumption was not significantly different between groups on postoperative day 1 or 2 (P > 0.05 in both cases). The frequency of side effects such as nausea and vomiting or respiratory depression was not significantly different between groups, but gabapentin was associated with decreased frequency of pruritus requiring nalbuphine (14% gabapentin vs. 43% control group, P < 0.001). The frequency of patients experiencing pain at 3 months post-thoracotomy was also comparable between groups (70% gabapentin vs. 66% placebo group, P = 0.72).
Conclusions: A single preoperative oral dose of gabapentin (600 mg) did not reduce pain scores or opioid consumption following elective thoracotomy, and did not confer any analgesic benefit in the setting of effective multimodal analgesia that included thoracic epidural infusion.
Trial registration: ClinicalTrials.gov NCT00588159.
© 2011 The Authors. Pain Practice © 2011 World Institute of Pain.
Figures
References
-
- Tan N, Agnew NM, Scawn ND, Pennefather SH, Chester M, Russell GN. Suprascapular nerve block for ipsilateral shoulder pain after thoracotomy with thoracic epidural analgesia: a double-blind comparison of 0.5% bupivacaine and 0.9% saline. Anesthesia & Analgesia. 2002;94:199–202. - PubMed
-
- Della Rocca G, Coccia C, Pompei L, Costa MG, Pierconti F, Di Marco P, et al. Post-thoracotomy analgesia: epidural vs intravenous morphine continuous infusion. Minerva Anestesiologica. 2002;68:681–693. - PubMed
-
- Mendola C, Ferrante D, Oldani E, Cammarota G, Cecci G, Vaschetto R, et al. Thoracic epidural analgesia in post-thoracotomy patients: comparison of three different concentrations of levobupivacaine and sufentanil. Br. J. Anaesth. 2009;102:418–423. - PubMed
-
- Cassivi SD, Allen MS, Vanderwaerdt GD, Ewoldt LL, Cordes ME, Wigle DA, et al. Patient-centered quality indicators for pulmonary resection. Annals of Thoracic Surgery. 2008;86:927–932. - PubMed
-
- Popping DM, Zahn PK, Van Aken HK, Dasch B, Boche R, Pogatzki-Zahn EM. Effectiveness and safety of postoperative pain management: a survey of 18 925 consecutive patients between 1998 and 2006 (2nd revision): a database analysis of prospectively raised data. British Journal of Anaesthesia. 2008;101:832–840. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
