

Early non-invasive cardiac output monitoring in hemodynamically unstable intensive care patients: a multi-center randomized controlled trial
- PMID: 21676229
- PMCID: PMC3219022
- DOI: 10.1186/cc10273
Early non-invasive cardiac output monitoring in hemodynamically unstable intensive care patients: a multi-center randomized controlled trial
Abstract
Introduction: Acute hemodynamic instability increases morbidity and mortality. We investigated whether early non-invasive cardiac output monitoring enhances hemodynamic stabilization and improves outcome.
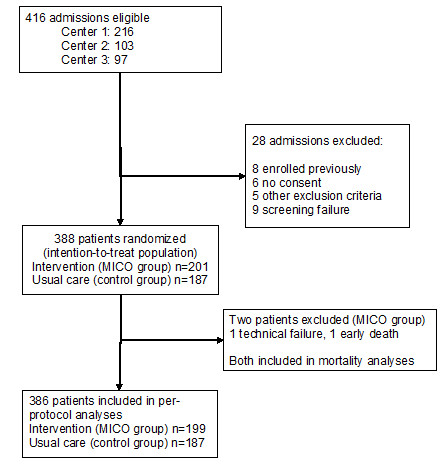
Methods: A multicenter, randomized controlled trial was conducted in three European university hospital intensive care units in 2006 and 2007. A total of 388 hemodynamically unstable patients identified during their first six hours in the intensive care unit (ICU) were randomized to receive either non-invasive cardiac output monitoring for 24 hrs (minimally invasive cardiac output/MICO group; n = 201) or usual care (control group; n = 187). The main outcome measure was the proportion of patients achieving hemodynamic stability within six hours of starting the study.
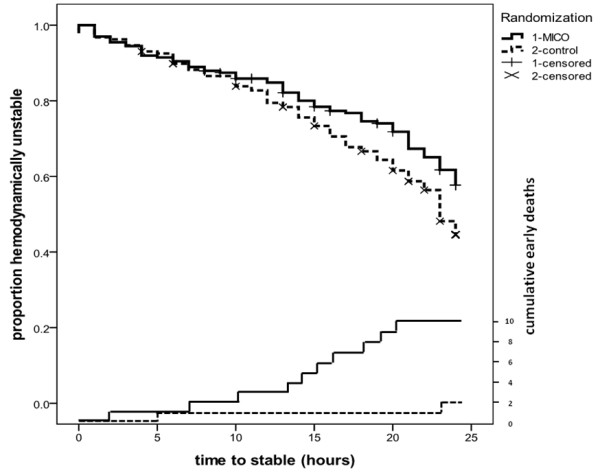
Results: The number of hemodynamic instability criteria at baseline (MICO group mean 2.0 (SD 1.0), control group 1.8 (1.0); P = .06) and severity of illness (SAPS II score; MICO group 48 (18), control group 48 (15); P = .86)) were similar. At 6 hrs, 45 patients (22%) in the MICO group and 52 patients (28%) in the control group were hemodynamically stable (mean difference 5%; 95% confidence interval of the difference -3 to 14%; P = .24). Hemodynamic support with fluids and vasoactive drugs, and pulmonary artery catheter use (MICO group: 19%, control group: 26%; P = .11) were similar in the two groups. The median length of ICU stay was 2.0 (interquartile range 1.2 to 4.6) days in the MICO group and 2.5 (1.1 to 5.0) days in the control group (P = .38). The hospital mortality was 26% in the MICO group and 21% in the control group (P = .34).
Conclusions: Minimally-invasive cardiac output monitoring added to usual care does not facilitate early hemodynamic stabilization in the ICU, nor does it alter the hemodynamic support or outcome. Our results emphasize the need to evaluate technologies used to measure stroke volume and cardiac output--especially their impact on the process of care--before any large-scale outcome studies are attempted.
Trial registration: The study was registered at ClinicalTrials.gov (Clinical Trials identifier NCT00354211).
Figures
Comment in
-
Should we use early less invasive hemodynamic monitoring in unstable ICU patients?Crit Care. 2011 Jul 28;15(4):173. doi: 10.1186/cc10287. Crit Care. 2011. PMID: 21888681 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
