

Results and current approach for Brachial Plexus reconstruction
- PMID: 21676269
- PMCID: PMC3127738
- DOI: 10.1186/1749-7221-6-2
Results and current approach for Brachial Plexus reconstruction
Abstract
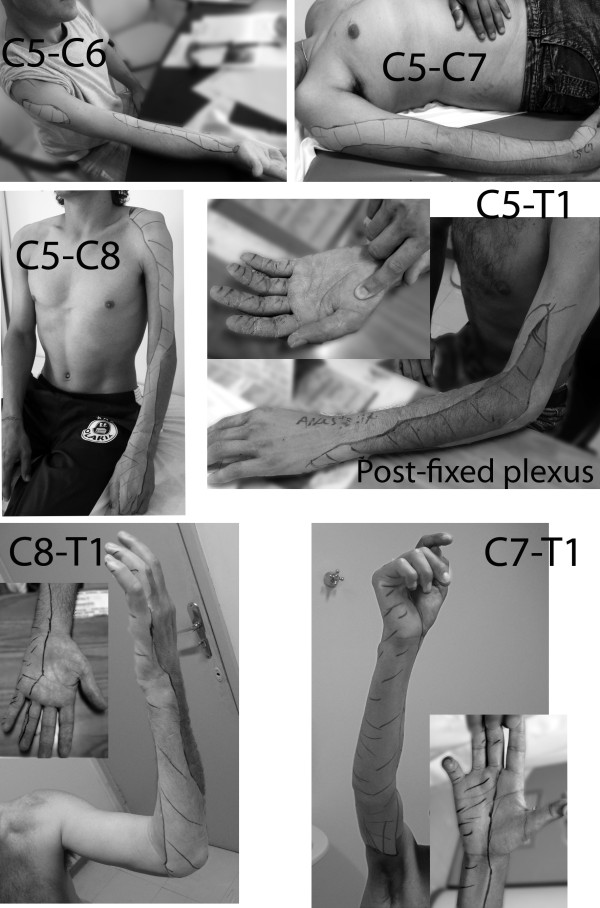
We review our experience treating 335 adult patients with supraclavicular brachial plexus injuries over a 7-year period at the University of Southern Santa Catarina, in Brazil. Patients were categorized into 8 groups, according to functional deficits and roots injured: C5-C6, C5-C7, C5-C8 (T1 Hand), C5-T1 (T2 Hand), C8-T1, C7-T1, C6-T1, and total palsy. To restore function, nerve grafts, nerve transfers, and tendon and muscle transfers were employed. Patients with either upper- or lower-type partial injuries experienced considerable functional return. In total palsies, if a root was available for grafting, 90% of patients had elbow flexion restored, whereas this rate dropped to 50% if no roots were grafted and only nerve transfers performed. Pain resolution should be the first priority, and root exploration and grafting helped to decrease or eliminate pain complaints within a short time of surgery.
Figures

References
-
- Robotti E, Longhi P, Verna G, Bocchiotti G. Brachial plexus surgery: an historical perspective. Hand Clin. 1995;6:517–533. - PubMed
-
- Bertelli JA, Ghizoni MF. Reconstruction of C5 and C6 brachial plexus avulsion injury by multiple nerve transfers: spinal accessory to suprascapular, ulnar fascicles to biceps branch, and triceps long or lateral head branch to axillary nerve. J Hand Surg Am. 2004;6:131–139. doi: 10.1016/j.jhsa.2003.10.013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous