

Early intervention for psychosis
- PMID: 21678345
- PMCID: PMC4163966
- DOI: 10.1002/14651858.CD004718.pub3
Early intervention for psychosis
Abstract
Background: Proponents of early intervention have argued that outcomes might be improved if more therapeutic efforts were focused on the early stages of schizophrenia or on people with prodromal symptoms. Early intervention in schizophrenia has two elements that are distinct from standard care: early detection, and phase-specific treatment (phase-specific treatment is a psychological, social or physical treatment developed, or modified, specifically for use with people at an early stage of the illness).Early detection and phase-specific treatment may both be offered as supplements to standard care, or may be provided through a specialised early intervention team. Early intervention is now well established as a therapeutic approach in America, Europe and Australasia.
Objectives: To evaluate the effects of: (a) early detection; (b) phase-specific treatments; and (c) specialised early intervention teams in the treatment of people with prodromal symptoms or first-episode psychosis.
Search strategy: We searched the Cochrane Schizophrenia Group Trials Register (March 2009), inspected reference lists of all identified trials and reviews and contacted experts in the field.
Selection criteria: We included all randomised controlled trials (RCTs) designed to prevent progression to psychosis in people showing prodromal symptoms, or to improve outcome for people with first-episode psychosis. Eligible interventions, alone and in combination, included: early detection, phase-specific treatments, and care from specialised early intervention teams. We accepted cluster-randomised trials but excluded non-randomised trials.
Data collection and analysis: We reliably selected studies, quality rated them and extracted data. For dichotomous data, we estimated relative risks (RR), with the 95% confidence intervals (CI). Where possible, we calculated the number needed to treat/harm statistic (NNT/H) and used intention-to-treat analysis (ITT).
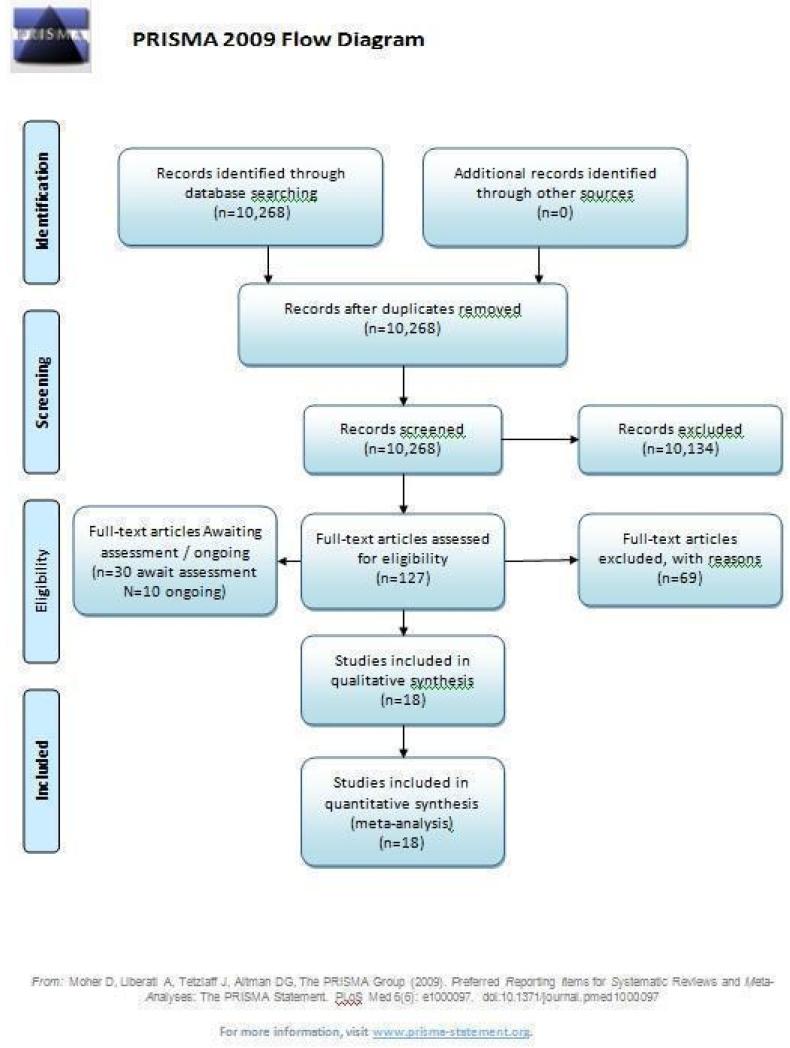
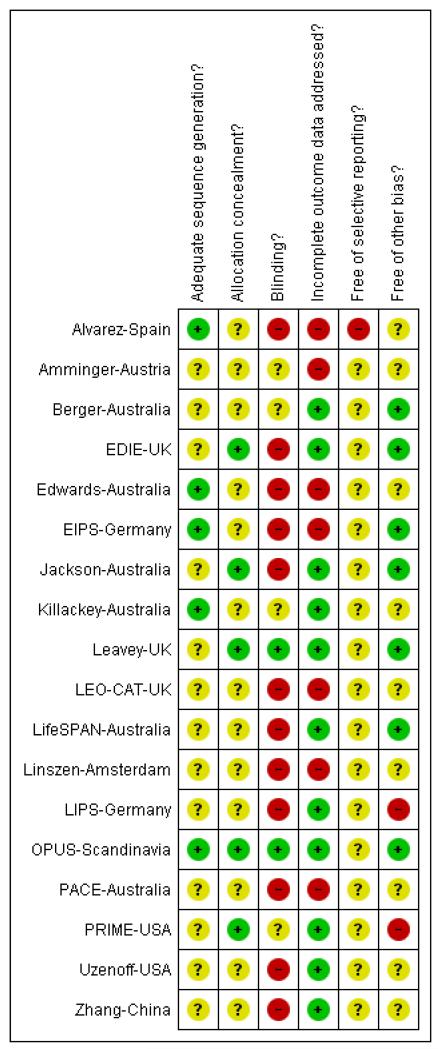
Main results: Studies were diverse, mostly small, undertaken by pioneering researchers and with many methodological limitations (18 RCTs, total n=1808). Mostly, meta-analyses were inappropriate. For the six studies addressing prevention of psychosis for people with prodromal symptoms, olanzapine seemed of little benefit (n=60, 1 RCT, RR conversion to psychosis 0.58 CI 0.3 to 1.2), and cognitive behavioural therapy (CBT) equally so (n=60, 1 RCT, RR conversion to psychosis 0.50 CI 0.2 to 1.7). A risperidone plus CBT plus specialised team did have benefit over specialist team alone at six months (n=59, 1 RCT, RR conversion to psychosis 0.27 CI 0.1 to 0.9, NNT 4 CI 2 to 20), but this was not seen by 12 months (n=59, 1 RCT, RR 0.54 CI 0.2 to 1.3). Omega 3 fatty acids (EPA) had advantage over placebo (n=76, 1 RCT, RR transition to psychosis 0.13 CI 0.02 to 1.0, NNT 6 CI 5 to 96). We know of no replications of this finding.The remaining trials aimed to improve outcome in first-episode psychosis. Phase-specific CBT for suicidality seemed to have little effect, but the single study was small (n=56, 1 RCT, RR suicide 0.81 CI 0.05 to 12.26). Family therapy plus a specialised team in the Netherlands did not clearly affect relapse (n=76, RR 1.05 CI 0.4 to 3.0), but without the specialised team in China it may (n=83, 1 RCT, RR admitted to hospital 0.28 CI 0.1 to 0.6, NNT 3 CI 2 to 6). The largest and highest quality study compared specialised team with standard care. Leaving the study early was reduced (n=547, 1 RCT, RR 0.59 CI 0.4 to 0.8, NNT 9 CI 6 to 18) and compliance with treatment improved (n=507, RR stopped treatment 0.20 CI 0.1 to 0.4, NNT 9 CI 8 to 12). The mean number of days spent in hospital at one year were not significantly different (n=507, WMD, -1.39 CI -2.8 to 0.1), neither were data for 'Not hospitalised' by five years (n=547, RR 1.05 CI 0.90 to 1.2). There were no significant differences in numbers 'not living independently' by one year (n=507, RR 0.55 CI 0.3 to 1.2). At five years significantly fewer participants in the treatment group were 'not living independently' (n=547, RR 0.42 CI 0.21 to 0.8, NNT 19 CI 14 to 62). When phase-specific treatment (CBT) was compared with befriending no significant differences emerged in the number of participants being hospitalised over the 12 months (n=62, 1 RCT, RR 1.08 CI 0.59 to 1.99).Phase-specific treatment E-EPA oils suggested no benefit (n=80, 1 RCT, RR no response 0.90 CI 0.6 to 1.4) as did phase-specific treatment brief intervention (n=106, 1 RCT, RR admission 0.86 CI 0.4 to 1.7). Phase-specific ACE found no benefit but participants given vocational intervention were more likely to be employed (n=41, 1 RCT, RR 0.39 CI 0.21 to 0.7, NNT 2 CI 2 to 4). Phase-specific cannabis and psychosis therapy did not show benefit (n=47, RR cannabis use 1.30 CI 0.8 to 2.2) and crisis assessment did not reduce hospitalisation (n=98, RR 0.85 CI 0.6 to 1.3). Weight was unaffected by early behavioural intervention.
Authors' conclusions: There is emerging, but as yet inconclusive evidence, to suggest that people in the prodrome of psychosis can be helped by some interventions. There is some support for specialised early intervention services, but further trials would be desirable, and there is a question of whether gains are maintained. There is some support for phase-specific treatment focused on employment and family therapy, but again, this needs replicating with larger and longer trials.
Figures
Update of
-
Early intervention for psychosis.Cochrane Database Syst Rev. 2006 Oct 18;(4):CD004718. doi: 10.1002/14651858.CD004718.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2011 Jun 15;(6):CD004718. doi: 10.1002/14651858.CD004718.pub3. PMID: 17054213 Updated.
Comment in
-
Review: more research needed on early intervention for psychosis.Evid Based Ment Health. 2012 Feb;15(1):23. doi: 10.1136/ebmh.2011.100201. Epub 2011 Nov 4. Evid Based Ment Health. 2012. PMID: 22058057 No abstract available.
References
References to studies included in this review
-
- Alvarez-Jimenez M, Gonzalez-Blanch C, Vazquez-Barquero JL, Perez-Iglesias R, Martinez-Garcia O, Perez-Pardal T, Ramírez-Bonilla ML, Crespo-Facorro B. Attenuation of antipsychotic-induced weight gain with early behavioral intervention in drug-naive first-episode psychosis patients: a randomized controlled trial. Journal of Clinical Psychiatry. 2006;67(8):1253–60. [EMBASE: 2006468531] - PubMed
- Alvarez M, Gonzalez-Blanch C, Perez-Iglesias R, Perez-Pardal T, Martinez-Garcia O, Crespo-Facorro B, Vazquez-Barquero JL. Early intervention in antipsychotic - induced weight gain in first episode psychosis. Schizophrenia Bulletin. 2005;31:518.
-
- Amminger G, Schaefer MR, Papageorgiou K, Becker J, Mossaheb N, Harrigan SM, McGorry PD, Berger GE. Omega-3 fatty acids reduce the risk of early transition to psychosis in ultra-high risk individuals: a double blind randomized, placebo-controlled treatment study. Schizophrenia Bulletin. 2007;33(2):418–9.
- Amminger GP. Indicated prevention with omega-3 fatty acids in adolescents with ‘at-risk-mental-state’ for psychosis: a randomised, double blind, placebo-controlled treatment trial. 2006 http://www.clinicaltrials.gov.
- Amminger GP, Schafer MR. Indicated prevention with omega-3 fatty acids in adolescents at ultra-high risk for psychosis - rationale, methods, and 3-months outcome. Schizophrenia Research. 2006;86(Suppl 1):S97–8.
- Amminger GP, Schafer MR. Is it feasible to conduct a RCT in ultra-high risk individuals at a child and adolescent psychiatric service? Schizophrenia Research. 2006;86(Suppl 1):S98.
- Schafer MR, Klier CM, Papageorgiou K, Friedrich MH, Amminger GP. Early detection of psychotic disorders. Neuropsychiatrie. 2007;21(1):37–44. - PubMed
-
- Berger G, Wood S, Proffitt T, Mcconchie M, Khan A, O’Donnell C, Yuen H, Smith D, Horrobin D, McGorry P. Ethyl-eicosapentaenoic acid (e-epa) supplementation in early psychosis. A double-blind randomized add on standard therapy study in 80 drug- native or early treated first episode psychosis patients. Schizophrenia Research. 2004;70(1):41. [: ISI:000224551100105]
- Berger GB, Proffitt TM, Mcconchie MA, Wood SJ, Yuen HP, Smith D, Horrobin D, McGorry PD. Ethyleicosapentaenoic acid (e-epa) supplementation in early psychosis. Schizophrenia Research. 2004;67(1):7–8. [: ISI 000188788100014]
- Berger GE, Proffitt T-M, McConchie M, Yuen H, Wood SJ, Amminger GP, Brewer W, McGorry PD. Ethyl-eicosapentaenoic acid in first-episode psychosis: a randomized, placebo-controlled trial. Journal of Clinical Psychiatry. 2007;68(12):1867–75. [MEDLINE: 18162017] - PubMed
- Berger GE, Proffitt TM, McConchie MA, Wood SJ, Yuen HP, McGorry PD. Ethyl - eicosapentaenoic acid (e - epa) supplementation in early psychosis. A double - blind, randomized, placebo - controlled trial (RCT) comparing 2g e - epa versus placebo add - on therapy in 80 drug - naive or early treated first - episode psychos. Schizophrenia Bulletin. 2005;31:475.
- Berger GE, Wood SJ, Wellard RM, Proffitt TM, McConchie M, Amminger GP, Jackson GD, Velakoulis D, Pantelis C, McGorry PD. Ethyl-eicosapentaenoic acid in first-episode psychosis. A 1H-MRS study. Neuropsychopharmacology. 2008;33(10):2467–73. [MEDLINE: 18199999] - PubMed
- Mcconchie MA, Berger GE, Proffitt TM, Yuen HP, Wood S, Smith D, Horrobin D, McGorry PD. Effect of diagnostic heterogeneity on response to ethyl- eicosapentaenoic acid (epa) in first-episode psychosis. Schizophrenia Research. 2004;67(1):147–8. [: ISI 000188788100352]
-
- French P, Shryane N, Bentall RP, Lewis SW, Morrison AP. Effects of cognitive therapy on the longitudinal development of psychotic experiences in people at high risk of developing psychosis. British Journal of Psychiatry - Supplementum. 2007;51:s82–7. - PubMed
- Lewis S. EDIE - Early detection and intervention for psychosis. National Research Register. 2001;Vol. 3
- Morrison A. Early detection and intervention for psychosis in primary care. National Research Register. 2003
- Morrison A. Follow-up of prodromal symptoms. National Research Register. 2004;Vol. 3
- Morrison AP. Cognitive therapy for the prevention of psychosis in people at ultra-high risk: results of a randomised controlled trial. Schizophrenia Research. 2006;86(Suppl 1):s59. - PubMed
- Morrison AP, Bentall RP, French P, Walford L, Kilcommons A, Knight A, Kreutz M, Lewis SW. Randomised controlled trial of early detection and cognitive therapy for preventing transition to psychosis in high-risk individuals. Study design and interim analysis of transition rate and psychological risk factors. British Journal of Psychiatry. 2002;43:s78–84. - PubMed
- Morrison AP, French P, Parker S, Roberts M, Stevens H, Bentall RP, Lewis SW. Three-year follow-up of a randomized controlled trial of cognitive therapy for the prevention of psychosis in people at ultrahigh risk. Schizophrenia Bulletin. 2007;33(3):682–7. [EMBASE: 2007428663; MEDLINE: 16973786; PSYCINFO: 2007–08119–011] - PMC - PubMed
-
*
- Morrison AP, French P, Walford L, Lewis SW, Kilcommons A, Green J, Parker S, Bentall RP. Cognitive therapy for the prevention of psychosis in people at ultra-high risk: randomised controlled trial. British Journal of Psychiatry. 2004;185:291–7. - PubMed
- Morrison T. Early detection and intervention for psychosis in primary care. National Research Register. 2001;Vol. 1
- Renton J, Morrison AP. Effectiveness of cognitive therapy for psychosis and implications for early intervention. Schizophrenia Research. 2004;70(1):142. [: ISI: 000224551100421]
-
- Edwards J, Elkins K, Hinton M, Harrigan SM, Donovan K, Athanasopoulos O, McGorry PD. Randomized controlled trial of a cannabis-focused intervention for young people with first-episode psychosis. Acta Psychiatrica Scandinavica. 2006;114:109–17. - PubMed
References to studies excluded from this review
-
- Addington J, Jones B, Ko T, Addington D. Family intervention in an early psychosis program. Psychiatric Rehabilitation Skills. In press.
- Addington J, Jones B, Ko T, Addington D. Intervention strategies for families of first episode patients. Proceedings of the Second International Conference on Early Psychosis; New York, USA. 2000 31st March - 2nd April.2000.
- Addington J, McCleery A, Addington D. Three-year outcome of family work in an early psychosis program. Schizophrenia Research. 2005;79(1):107–16. - PubMed
-
- Agius M, Shah S, Ramkisson R, Murphy S, Zaman R. Three-year outcomes of an early intervention for psychosis service as compared with treatment as usual for first psychotic episodes in a standard community mental health team - final results. Psychiatria Danubina. 2007;19(3):130–8. [MEDLINE: 17914313] - PubMed
-
- Alanen YO, Lehtinen V, Lehtinen K, Aaltonen J, Rakkolainen V. In: The Finnish Integrated Model for Early Treatment of Schizophrenia and Related Psychoses. Martindale B, Bateman A, editors. Gaskell/Royal College of Psychiatrists; London, England: 2000. pp. 235–65.
- Alanen YO, Ugelstad E, Armelius BA, Lehtinen K, Rosenbaum B, Sjostrom R. Early Treatment for Schizophrenic Patients: Scandinavian Psychotherapeutic Approach. Scandinavian University Press; Oslo: 1994.
- Lehtinen K, Tuori T, Jaaskelain NJ. Using psychosis teams in early intervention. A follow-up study of the Finnish schizophrenia project. Nordic Journal of Psychiatry. 1998;52(Suppl):74.
- Lehtinen V, Aaltonen J, Koffert T, Rakkolainen V, Syvalahti E. Two-year outcome in first-episode psychosis treated according to an integrated model. Is immediate neuroleptisation always needed? European Psychiatry. 2000;15:312–20. - PubMed
-
- Albiston D, Francey SM, Harrigan SM. Group programmes for recovery from early psychosis. British Journal of Psychiatry. 1998;172(33):117–21. - PubMed
-
- Anonymous. The Scottish first episode schizophrenia study. ii. Treatment: pimozide versus flupenthixol. British Journal of Psychiatry. 1987;150:334–8. - PubMed
References to studies awaiting assessment
-
- Addington J, Addington D. Impact of an early psychosis program on substance use. Journal of Psychiatric Rehabilitation. 2001;25(1):60–7. - PubMed
-
- Alaghband-rad J, Shahrivar Z, Mahmoodi J, Salesian N. First episode psychoses among Iranian adolescents. Schizophrenia Research. 2006;86(Suppl 1):S65.
- Alaghband-Rad J, Sharifi V, Amini H, Shahrivar Z, Mottaghipour Y, Mahmoodi J, Seddigh A, Salesian N, Ali-Malayeri A, Tabatabaee M. Management of first episode psychoses in Iran: unique features and challenges. Schizophrenia Research. 2006;86(Suppl 1):S42.
-
- Berger G. Lithium in patients at ultra high risk of developing a first psychotic episode. Stanley Foundation Research Programs; 2006.
-
- Cornblatt B. Risperidone vs sertraline for prodromal schizophrenia. Stanley Foundation Research Programs; 2009.
- NCT00169988 Sertraline alone vs in combination with risperidone in the treatment of attenuated positive and negative symptoms. 2005 http://www.clinicaltrials.gov.
-
- Dai M, Liu F, Fan J. A study on influence of early comprehensive interventions on prognosis of incipient schizophrenia patients. Chinese Nursing Research. 2007;21:2393–4.
References to ongoing studies
-
- Addington J, Christensen B, Remington G, Lau M, Monette G. A randomized controlled trial of individual therapy for first episode psychosis. http://www.clinicaltrials.gov.
-
- Arends J. Prodromal symptoms and early intervention to prevent a relapse. 2006 http://www.controlled-trials.com/
-
- Morrison AP. EDIE-2: early detection and psychological intervention for individuals at high risk of psychosis (2) Current Controlled Trials. 2007
- Morrison T. Early detection and psychological intervention for individuals at high risk of psychosis. EDIE-2. Data on file 2006.
-
- Furimsky I, Mcmillan S, Zipursky RB, Addington J, Dewa C, Boydell K, Noh S. Access, detection and psychological treatments. http://www.clinicaltrials.gov.
-
- Gaebel W. Prodrome-based early intervention with antipsychotics vs benzodiazepine in patients with first-episode schizophrenia after one year maintenance treatment under further maintenance treatment vs stepwise discontinued drugs. http://www.clinicaltrials.gov.
- Gaebel W. Maintenance treatment vs stepwise drug discontinuation after one year of maintenance treatment in first-episode schizophrenia. http://www.clinicaltrials.gov.
Additional references
-
- Addington D, Addington J, Schissel B. A depression rating scale for schizophrenics. Schizophrenia Research. 1990;3:247–25. - PubMed
-
- Andreasen NC. Schedule for the Assessment of Negative Symptoms. University of Iowa; Iowa City, Iowa: 1983.
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 4th Edition APA; Washington, DC: 1994.
-
- Barnes TR. A rating scale for drug-induced akathisia. British Journal of Psychiatry. 1989;154:672–6. - PubMed
References to other published versions of this review
-
- Marshall M, Lockwood A. Early Intervention for psychosis. Cochrane Database of Systematic Reviews. 2004;(Issue 2) [DOI: 10.1002/14651858.CD004718] - PubMed
-
-
* Indicates the major publication for the study
-
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous