

New insights into insulin resistance in the diabetic heart
- PMID: 21680199
- PMCID: PMC3183400
- DOI: 10.1016/j.tem.2011.05.001
New insights into insulin resistance in the diabetic heart
Abstract
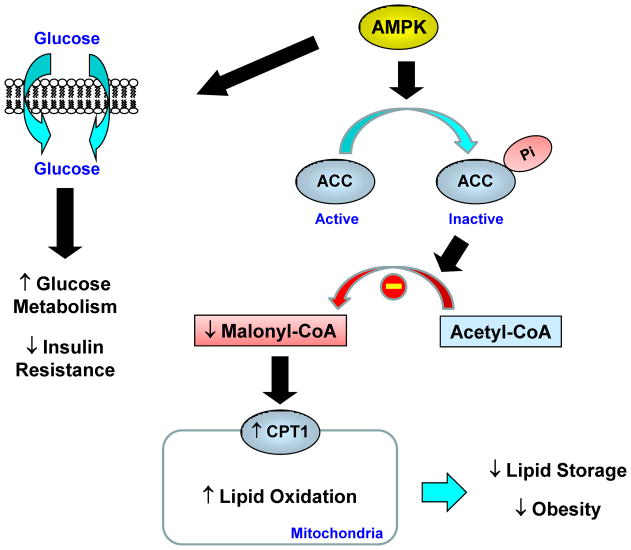
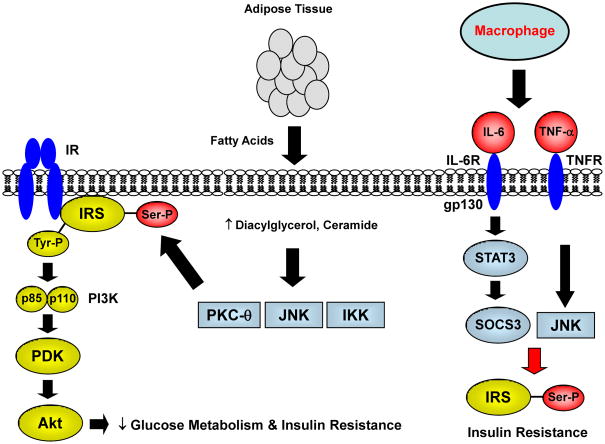
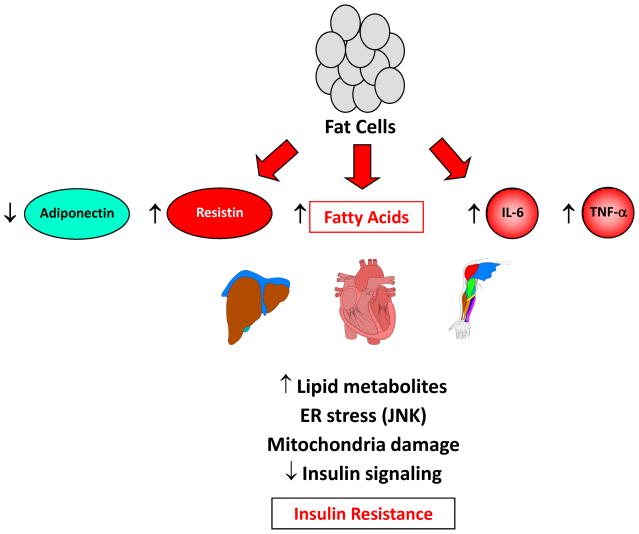
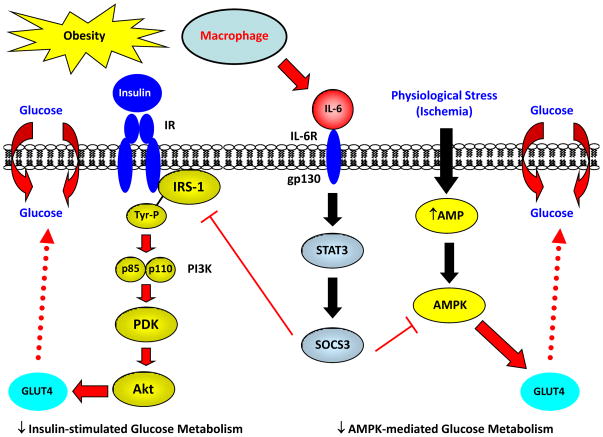
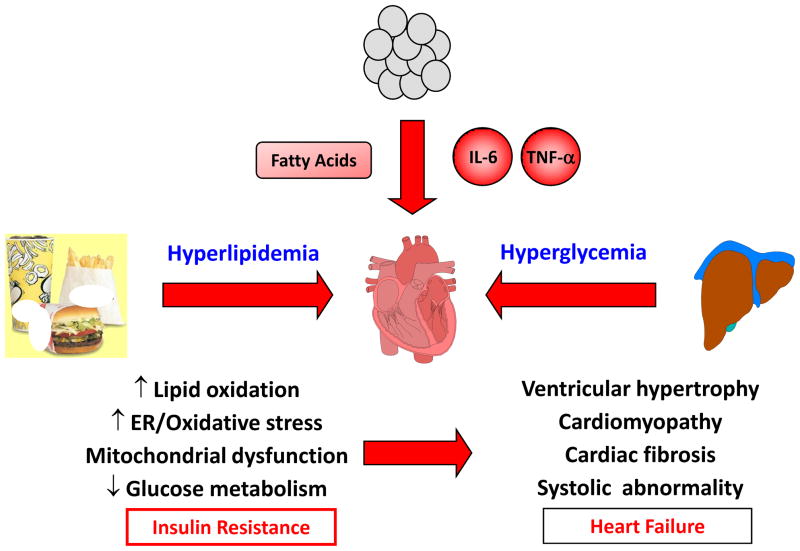
Insulin resistance is a major characteristic of obesity and type 2 diabetes, and develops in multiple organs, including the heart. Compared with its role in other organs, the physiological role of insulin resistance in the heart is not well understood. The heart uses lipid as a primary fuel, but glucose becomes an important source of energy in ischemia. The impaired ability to utilize glucose might contribute to cell death and abnormal function in the diabetic heart. Recent discoveries regarding the role of inflammation, mitochondrial dysfunction and endoplasmic reticulum (ER) stress in obesity have advanced our understanding of how insulin resistance develops in peripheral organs. In this review, we examine these findings in relation to the diabetic heart to provide new insights into the mechanism of cardiac insulin resistance.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Wild S, et al. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- Grundy SM, et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999;100:1134–1146. - PubMed
-
- Bell DS. Heart failure: the frequent, forgotten, and often fatal complication of diabetes. Diabetes Care. 2003;26:2433–2441. - PubMed
-
- Boyer JK, et al. Prevalence of ventricular diastolic dysfunction in asymptomatic normotensive patients with diabetes mellitus. Am J Cardiol. 2004;93:870–875. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
