

Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study
- PMID: 21680910
- PMCID: PMC3632011
- DOI: 10.1093/jnci/djr203
Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study
Erratum in
- J Natl Cancer Inst. 2013 Apr 17;105(8):581
Abstract
Background: Barrett's esophagus (BE) is a premalignant lesion that predisposes to esophageal adenocarcinoma. However, the reported incidence of esophageal adenocarcinoma in patients with BE varies widely. We examined the risk of malignant progression in patients with BE using data from the Northern Ireland Barrett's esophagus Register (NIBR), one of the largest population-based registries of BE worldwide, which includes every adult diagnosed with BE in Northern Ireland between 1993 and 2005.
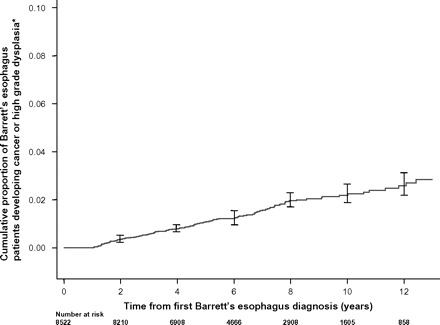
Subjects and methods: We followed 8522 patients with BE, defined as columnar lined epithelium of the esophagus with or without specialized intestinal metaplasia (SIM), until the end of 2008. Patients with incident adenocarcinomas of the esophagus or gastric cardia or with high-grade dysplasia of the esophagus were identified by matching the NIBR with the Northern Ireland Cancer Registry, and deaths were identified by matching with records from the Registrar General's Office. Incidence of cancer outcomes or high-grade dysplasia was calculated as events per 100 person-years (% per year) of follow-up, and Cox proportional hazard models were used to determine incidence by age, sex, length of BE segment, presence of SIM, macroscopic BE, or low-grade dysplasia. All P values were from two-sided tests.
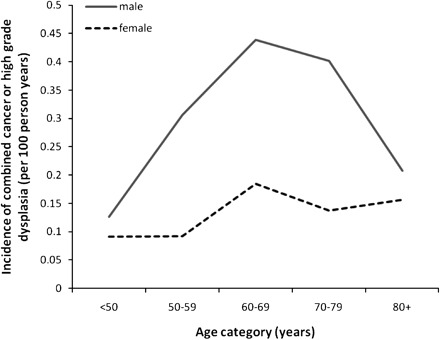
Results: After a mean of 7.0 years of follow-up, 79 patients were diagnosed with esophageal cancer, 16 with cancer of the gastric cardia, and 36 with high-grade dysplasia. In the entire cohort, incidence of esophageal or gastric cardia cancer or high-grade dysplasia combined was 0.22% per year (95% confidence interval [CI] = 0.19% to 0.26%). SIM was found in 46.0% of patients. In patients with SIM, the combined incidence was 0.38% per year (95% CI = 0.31 to 0.46%). The risk of cancer was statistically significantly elevated in patients with vs without SIM at index biopsy (0.38% per year vs 0.07% per year; hazard ratio [HR] = 3.54, 95% CI = 2.09 to 6.00, P < .001), in men compared with women (0.28% per year vs 0.13% per year; HR = 2.11, 95% CI = 1.41 to 3.16, P < .001), and in patients with low-grade dysplasia compared with no dysplasia (1.40% per year vs 0.17% per year; HR = 5.67, 95% CI = 3.77 to 8.53, P < .001).
Conclusion: We found the risk of malignant progression among patients with BE to be lower than previously reported, suggesting that currently recommended surveillance strategies may not be cost-effective.
Figures
Comment in
-
Understanding cancer incidence in Barrett's esophagus: light at the end of the tunnel.J Natl Cancer Inst. 2011 Jul 6;103(13):994-5. doi: 10.1093/jnci/djr223. Epub 2011 Jun 16. J Natl Cancer Inst. 2011. PMID: 21680911 No abstract available.
-
Re: Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study.J Natl Cancer Inst. 2012 Nov 21;104(22):1771-2. doi: 10.1093/jnci/djs426. Epub 2012 Oct 4. J Natl Cancer Inst. 2012. PMID: 23042934 No abstract available.
References
-
- Steevens J, Botterweck AA, Dirx MJ, van den Brandt PA, Schouten LJ. Trends in incidence of oesophageal and stomach cancer subtypes in Europe. Eur J Gastroenterol Hepatol. 2010;22(6):669–678. - PubMed
-
- Eloubeidi MA, Mason AC, Desmond RA, El-Serag HB. Temporal trends (1973-1997) in survival of patients with esophageal adenocarcinoma in the United States: a glimmer of hope? Am J Gastroenterol. 2003;98(7):1627–1633. - PubMed
-
- US National Cancer Institute. SEER Stat Fact Sheets: Esophagus. 2010. http://seer.cancer.gov/statfacts/html/esoph.html - survival. Accessed October 5, 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
