

Topographical continuity of bacterial populations in the healthy human respiratory tract
- PMID: 21680950
- PMCID: PMC3208663
- DOI: 10.1164/rccm.201104-0655OC
Topographical continuity of bacterial populations in the healthy human respiratory tract
Abstract
Rationale: Defining the biogeography of bacterial populations in human body habitats is a high priority for understanding microbial-host relationships in health and disease. The healthy lung was traditionally considered sterile, but this notion has been challenged by emerging molecular approaches that enable comprehensive examination of microbial communities. However, studies of the lung are challenging due to difficulties in working with low biomass samples.
Objectives: Our goal was to use molecular methods to define the bacterial microbiota present in the lungs of healthy individuals and assess its relationship to upper airway populations.
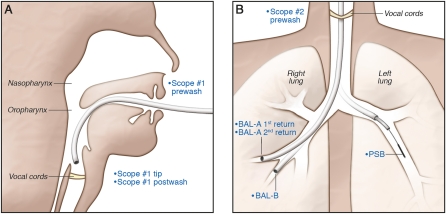
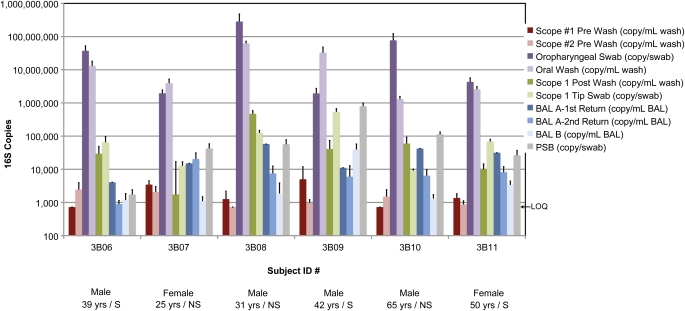
Methods: We sampled respiratory flora intensively at multiple sites in six healthy individuals. The upper tract was sampled by oral wash and oro-/nasopharyngeal swabs. Two bronchoscopes were used to collect samples up to the glottis, followed by serial bronchoalveolar lavage and lower airway protected brush. Bacterial abundance and composition were analyzed by 16S rDNA Q-PCR and deep sequencing.
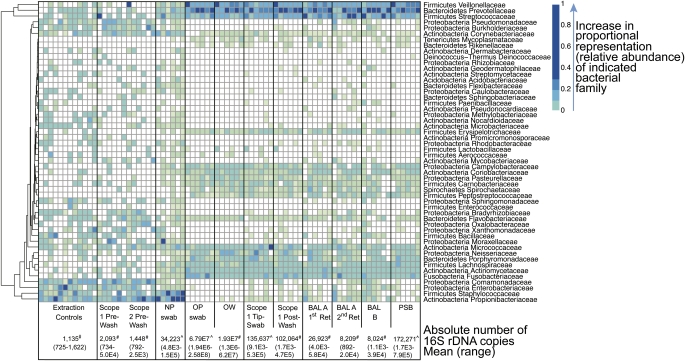
Measurements and main results: Bacterial communities from the lung displayed composition indistinguishable from the upper airways, but were 2 to 4 logs lower in biomass. Lung-specific sequences were rare and not shared among individuals. There was no unique lung microbiome.
Conclusions: In contrast to other organ systems, the respiratory tract harbors a homogenous microbiota that decreases in biomass from upper to lower tract. The healthy lung does not contain a consistent distinct microbiome, but instead contains low levels of bacterial sequences largely indistinguishable from upper respiratory flora. These findings establish baseline data for healthy subjects and sampling approaches for sequence-based analysis of diseases.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
