

Outcomes of antiretroviral treatment in programmes with and without routine viral load monitoring in Southern Africa
- PMID: 21681057
- PMCID: PMC3605707
- DOI: 10.1097/QAD.0b013e328349822f
Outcomes of antiretroviral treatment in programmes with and without routine viral load monitoring in Southern Africa
Abstract
Objectives: To compare outcomes of antiretroviral therapy (ART) in South Africa, where viral load monitoring is routine, with those in Malawi and Zambia, where monitoring is based on CD4 cell counts.
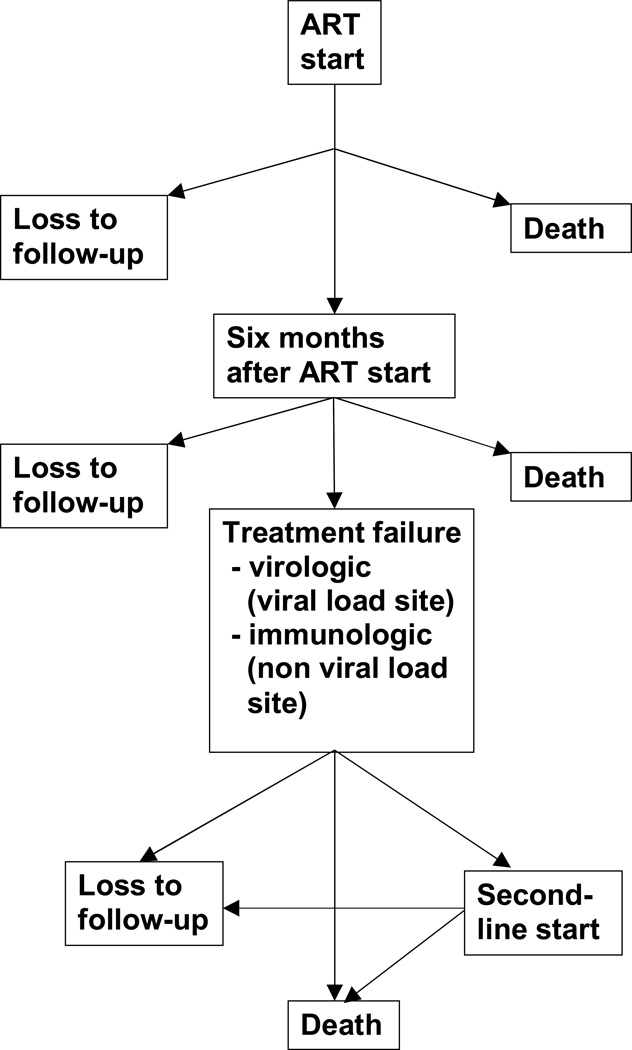
Methods: We included 18,706 adult patients starting ART in South Africa and 80,937 patients in Zambia or Malawi. We examined CD4 responses in models for repeated measures and the probability of switching to second-line regimens, mortality and loss to follow-up in multistate models, measuring time from 6 months.
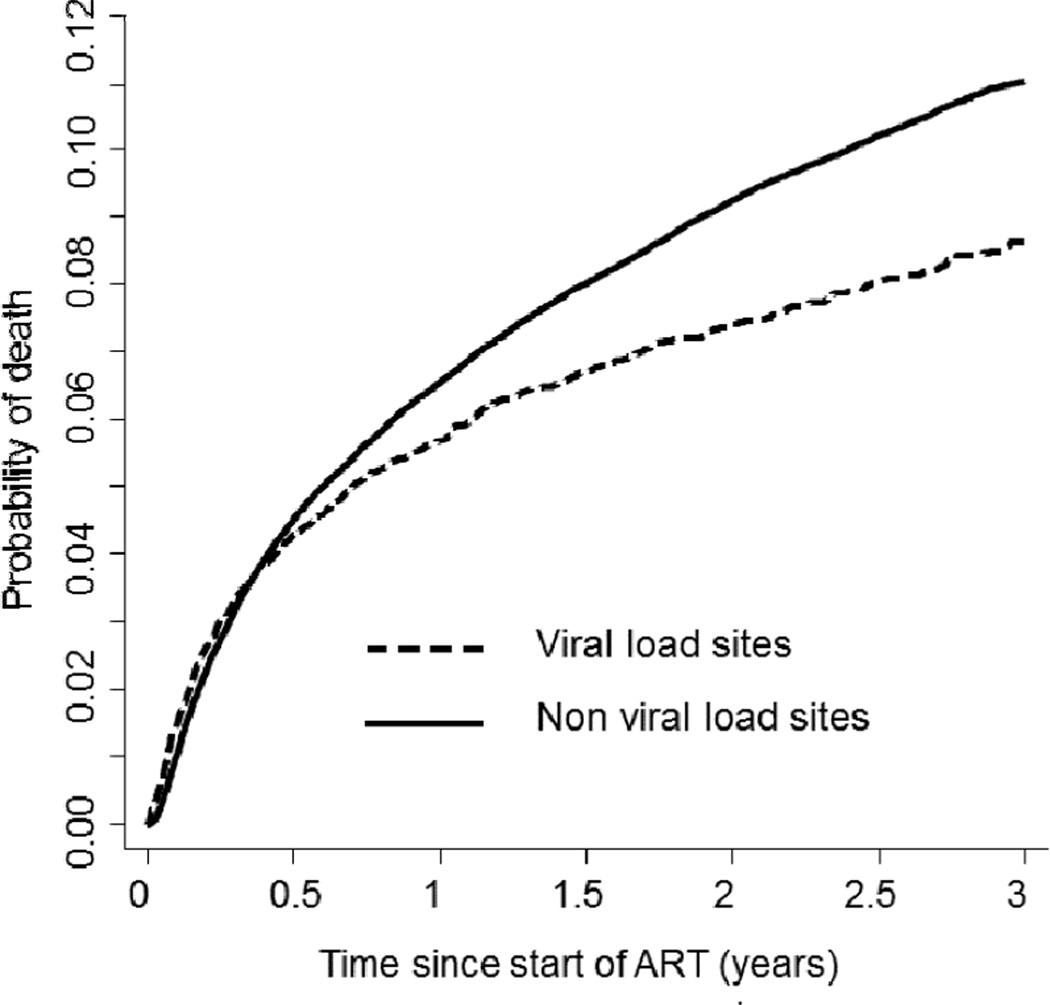
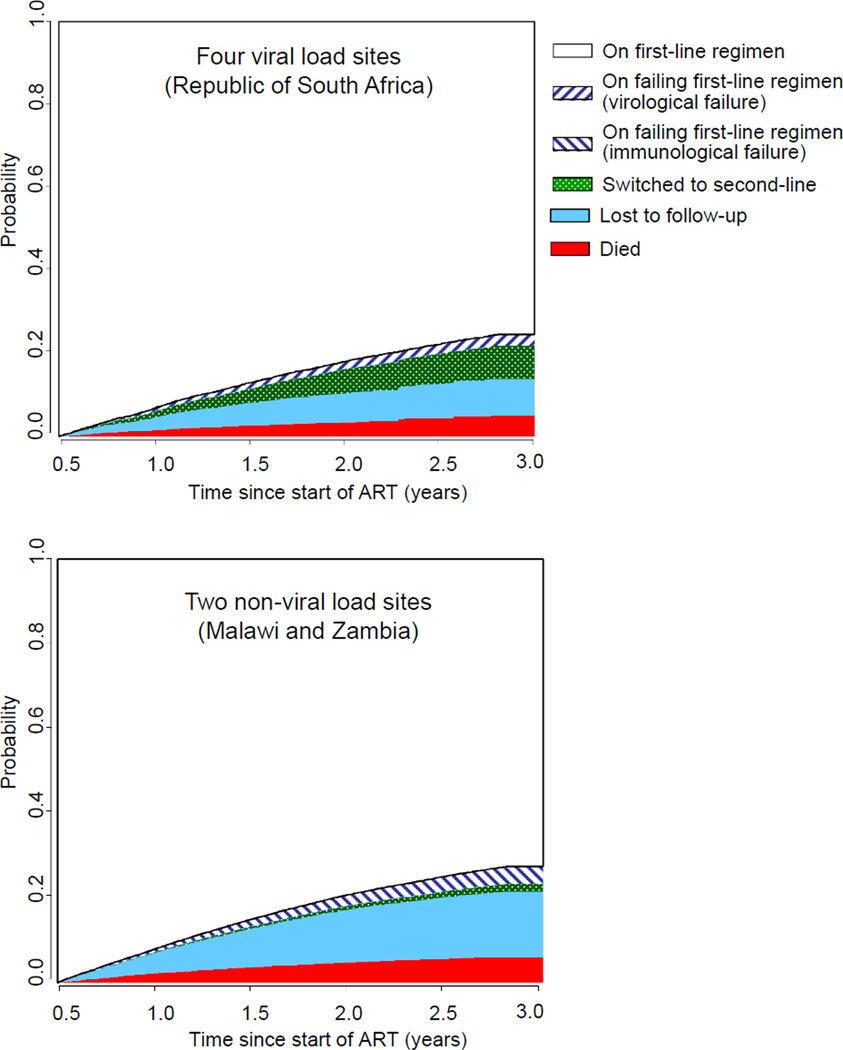
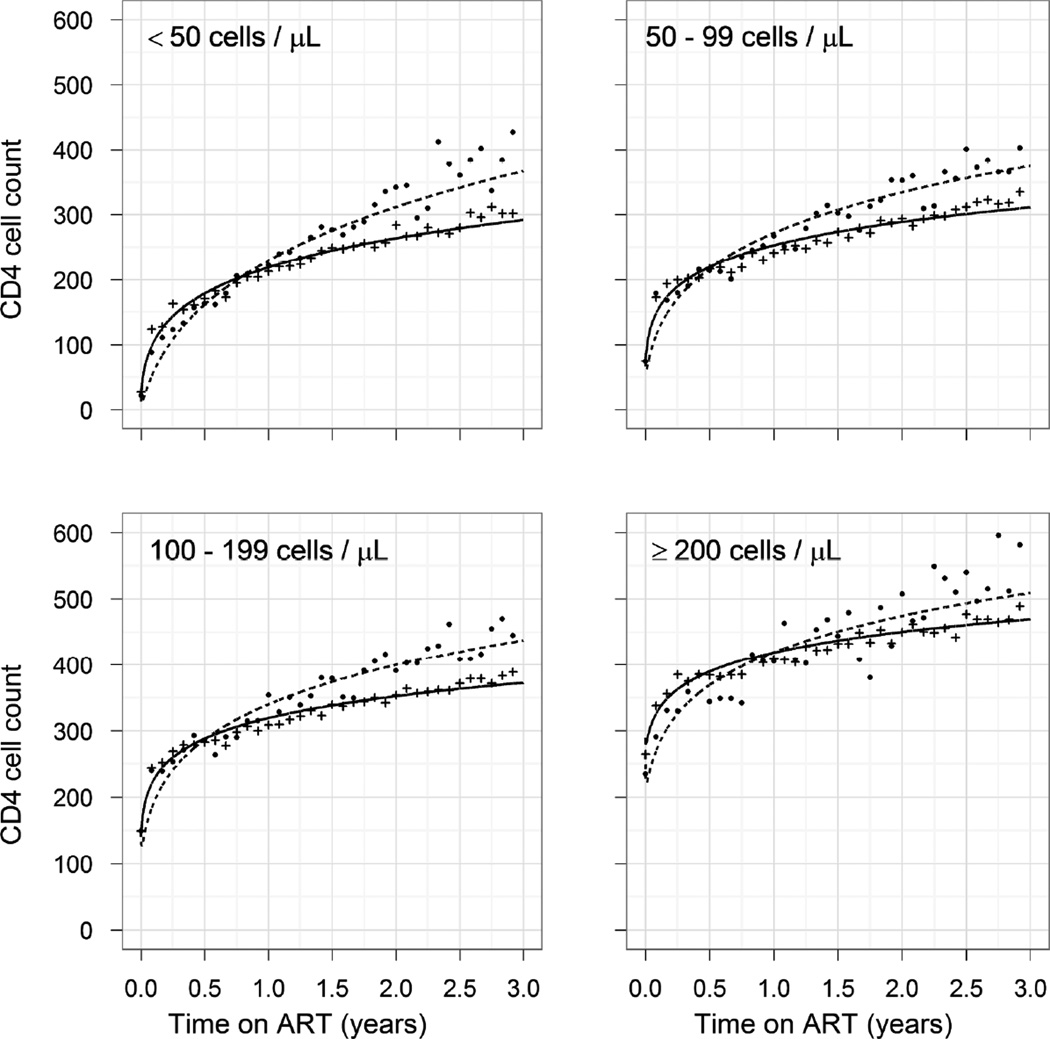
Results: In South Africa, 9.8% [95% confidence interval (CI) 9.1-10.5] had switched at 3 years, 1.3% (95% CI 0.9-1.6) remained on failing first-line regimens, 9.2% (95% CI 8.5-9.8) were lost to follow-up and 4.3% (95% CI 3.9-4.8) had died. In Malawi and Zambia, more patients were on a failing first-line regimen [3.7% (95% CI 3.6-3.9], fewer patients had switched [2.1% (95% CI 2.0-2.3)] and more patients were lost to follow-up [15.3% (95% CI 15.0-15.6)] or had died [6.3% (95% CI 6.0-6.5)]. Median CD4 cell counts were lower in South Africa at the start of ART (93 vs. 132 cells/μl; P < 0.001) but higher after 3 years (425 vs. 383 cells/μl; P < 0.001). The hazard ratio comparing South Africa with Malawi and Zambia after adjusting for age, sex, first-line regimen and CD4 cell count was 0.58 (0.50-0.66) for death and 0.53 (0.48-0.58) for loss to follow-up.
Conclusion: Over 3 years of ART mortality was lower in South Africa than in Malawi or Zambia. The more favourable outcome in South Africa might be explained by viral load monitoring leading to earlier detection of treatment failure, adherence counselling and timelier switching to second-line ART.
Figures
References
-
- World Health Organization. Progress Report 2010. Geneva: World Health Organization; 2010. [Accessed 20 May 2011]. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. Available at http://www.who.int/hiv/pub/2010progressreport/en/index.html.
-
- World Health Organization. 2010 revision. Geneva: World Health Organization; 2010. [Accessed 20 May 2011]. Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. Available at http://www.who.int/hiv/pub/arv/adult2010/en/index.html. - PubMed
-
- Moore DM, Mermin J, Awor A, Yip B, Hogg RS, Montaner JS. Performance of immunologic responses in predicting viral load suppression: implications for monitoring patients in resource-limited settings. J Acquir Immune Defic Syndr. 2006;43:436–439. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
